Ladda ner presentationen
Presentation laddar. Vänta.

1
PERIOPERATIV DIABETES KONTROLL
O. Naesh, docent Anestesi-Intensivvård-Smärtenheten Helsingborgs Lasarett

2
Vi har ett problem…. Ålder Diabetes Metabolt syndr. 2000 2010 2020
Vi har ett problem…. Diabetes Metabolt syndr. O.Naesh

3
Non-insulin dependent
Typ 1 3 % Typ 2 6 -10 % Insulin dependent Non-insulin dependent Metabolt syndrom BMI > 30 Katabolism Stress Periop. Risk Infektion Sårheling Ischemiska skador Dehydrering B-Glukos < mmol/L O.Naesh

4
Lipshutz Anesthesiology 2009; 110:408–21

5
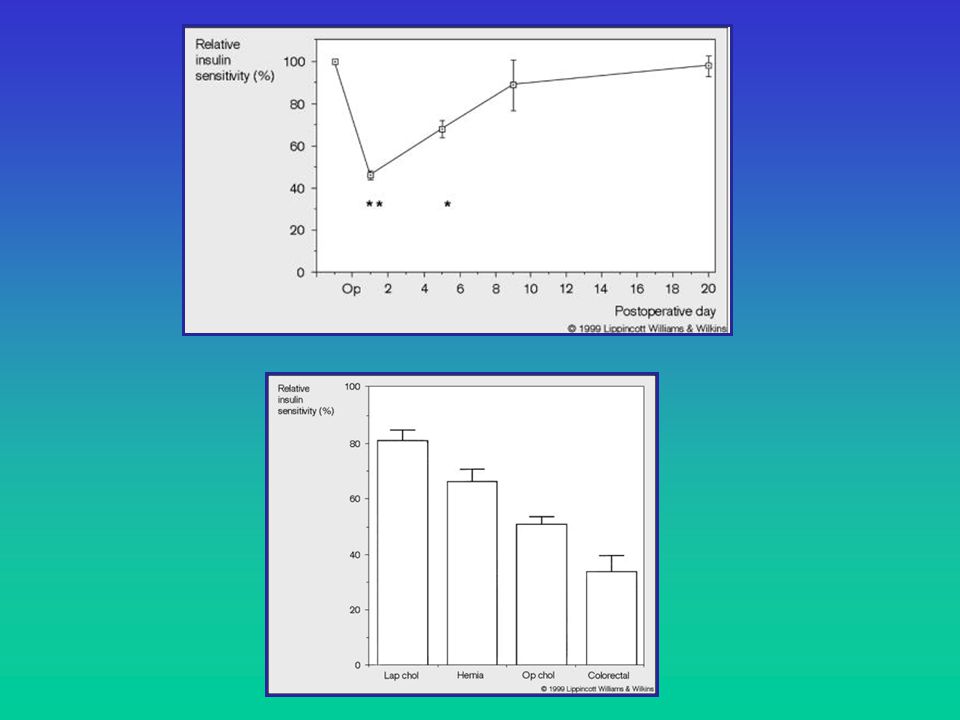
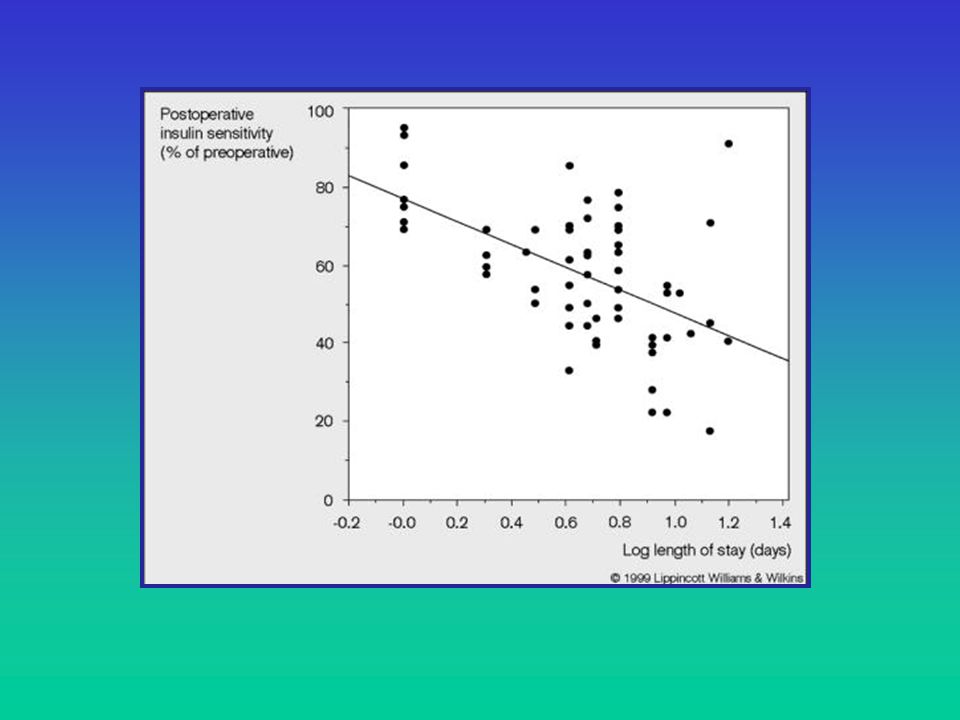
Den Perioperativa Patienten
Kir. Traum Hälsostatus Diet HPA respons Inflam.mediatorer Immobilisering GLUT4 translokation Glykogena hormon Glykogena hormon GLUT4 FFA & Metaboliter Post-receptor signal PI-3 kinas INSULIN RESISTANS

6
KIRURGISK STRESS RESPONS
Protektivt / Överlevnads Respons Sympatikus Neuro-endokrint Immunologisk / Inflammatorisk Substrat mobilisering (katabolism) Akut fas respons Lipid Metabolism GLUKOS OP dagar Monoaminer, peptider, transcriptionsfaktorer Genom ändringar CRH, synapseffekter corticosteroider O.Naesh
 Akut fas respons. Lipid Metabolism. GLUKOS. OP dagar. Monoaminer, peptider, transcriptionsfaktorer Genom ändringar. CRH, synapseffekter corticosteroider. O.Naesh.")
7
Mitokondrie Dysfunktion
GLUKOS STRESS RESPONSE GLUT - Glukos GLUT Insulin avhängig Muskel Myocardium Adipocyter Insulin oavhängig INSULIN RESISTENS Immun Dysfunktion Endothel Dysfunktion Myokard Dysfunktion Mitokondrie Dysfunktion CNS Dysfunktion Glukos Overload Glukos Toxicitet Oxidativt stress Fria Radikal O.Naesh

8
INSULIN - Glukos Overload Ischemi/Reperf. Skada Anti -inflammatorisk
Insulin oavhängig Glukos Overload Glukos Toxicitet Oxidativt stress Fria Radikal - Anti -inflammatorisk Lipid normalisering Endothel protektion Anabolism Sårheling Ischemi/Reperf. Skada INSULIN O.Naesh

11
INTENSIVE INSULIN THERAPY IN CRITICALLY ILL PATIENTS
GREET VAN DEN BERGHE, M.D., PH.D., PIETER WOUTERS, M.SC., FRANK WEEKERS, M.D., CHARLES VERWAEST, M.D., FRANS BRUYNINCKX, M.D., MIET SCHETZ, M.D., PH.D., DIRK VLASSELAERS, M.D., PATRICK FERDINANDE, M.D., PH.D., PETER LAUWERS, M.D., AND ROGER BOUILLON, M.D., PH.D NEJM 2001;345(19):1359 B-Glukos < 5,5 mmol/L vs < 11 mmol/L
:1359. B-Glukos < 5,5 mmol/L vs < 11 mmol/L.")
12
Flertallet studier visar att….
“Tight” Blodsocker Kontroll / Normoglykemi…… (< 6,1 vs < 8,3 vs > 8,5) ~ % reduktion i mortalitet / morbiditet (IVA patienter / Hjärt-Kärl kirurgi och AMI) ……..få studier av Generell Kirurgi Glycaemic control and perioperative organ protection. G.van den Berghe et al. Best Practice & Research Clinical Anaesthesiology Vol. 22, No. 1, pp. 135–149, 2008 O.Naesh
 ~ % reduktion i mortalitet / morbiditet. (IVA patienter / Hjärt-Kärl kirurgi och AMI) ……..få studier av Generell Kirurgi. Glycaemic control and perioperative organ protection. G.van den Berghe et al. Best Practice & Research Clinical Anaesthesiology Vol. 22, No. 1, pp. 135–149, O.Naesh.")
13
Metod till Perioperativ Blod Socker Kontrol
Kontinuerlig Insulin i Pump + Separat Glukos Infusion Glukos - Insulin Drop Subcutan Insulin + Glukos 2.5 % O.Naesh

14
Metoder vid 31 svenska anestesi kliniker
Övre accept gräns Mätt interval mmol/L 12 10 8 6 4 2 mmol/L 100 % > ’ ’ tim 100 % I.v S.c S.c+I.v. Insulin tillförsel < 50 % har skrivna riktlinjer…. O.Naesh

15
PRO CON Kontinuerlig Insulin i Pump + Separat Glukos Infusion
Säkrer adekvat Hypoglykemi insulin mängd Kontinuerlig Insulin i Pump + Separat Glukos Infusion Enkelt Ej Styrbart Glukos tillförsel Ofta inadekvat Glukos - Insulin Drop Subcutan Insulin + Glukos 2.5 % Ofta adekvat vid Typ Ej fin-styrning och kir. minor O.Naesh

16
Breaking News ! B-Glukos 10 Glycemic Control for Organs
Anesthesiology 2009; 110:204–6 Perioperative Glucose Control What Is Enough? The New England Journal of Medicine March 26, 2009 vol. 360 no. 13 Intensive versus Conventional Glucose Control in Critically Ill Patients The NICE-SUGAR Study Investigators* (N = 6104) Anesthesiology 2009; 110:207–8 Glycemic Control for Organs A New Approach to a Controversial Topic ?? Extrapolera från Intensivvård till perioperativt ?? B-Glukos 4,5 -6,0 …”för tight” - ökad risk för hypoglykemi och ökad mortalitet - NNH = 38 B-Glukos 10 O.Naesh
 Anesthesiology 2009; 110:207–8. Glycemic Control for Organs. A New Approach to a Controversial Topic. Extrapolera från Intensivvård till perioperativt B-Glukos 4,5 -6,0 … för tight - ökad risk för hypoglykemi och ökad mortalitet - NNH = 38. B-Glukos 10. O.Naesh.")
17
NICE-SUGAR Study NEJM 2009;360(13):1283 Target B-Glucose: 4,5 vs. 10 mmol/L
:1283 Target B-Glucose: 4,5 vs. 10 mmol/L")
18
Blod Socker koncentrationer mellan
MÅLSÄTTNING Blod Socker Kontrol under den perioperativa period Blod Socker koncentrationer mellan > 6 och < 10 mmol/L Lagom Sött… Minimera risk för hypoglykemi -alltid insulin + Glukos 10% infusion ! Täta mätningar ! Löpande justeringar ! O.Naesh

19
A: KOSTBEHANDLING ELLER PERORALT ANTI-DIABETIKUM
PERIOPERATIV DIABETESBEHANDLING (Vuxna) OBS! Under pågående behandling enl. detta PM är all annan ordinerad antidiabetisk behandling tillfälligt seponerad ! Sätt alltid 10 % Glukos med (Na+/K+=40/20 mmol) i samband med insulin infusion ! A: KOSTBEHANDLING ELLER PERORALT ANTI-DIABETIKUM A1: Mindre kirurgi/Dagkirurgi: Fasta 6 tim preop. (2 tim för vatten) Inga perorala antidiabetika < 12 timmar innan Op. P-Glukos vid ankomst Om P-Glukos < 6 mmol/L: sätt 1000 ml Buffrad Glukos 25 mg/ml (83 ml/tim) Om P-Glukos 6 – 14 mmol/L: sätt 1000 ml Ringer Acetat Om P-Glukos > 14 mmol/L: Kontakta ansv. anestesiolog för ställningstagande till om operationen kan uppskjutas eller om insulininfusion + 10 % Glukos + (NA+/K+= 40/20 mmol) ska startas (enl. algoritm) Mät P-Glukos varannan timme tills födointag A2: Större Kirurgi (inneliggande): P-Glukos kvällen före op. (om > 12 mol/L kontakta anestesiolog 62160) Fasta 6 tim preop. (2 tim för vatten/nutritions dryck) Inga perorala antidiabetika < 12 timmar innan op. P-Glukos kl. 06:00 på op-dagen Om P-Glukos < 6 mmol/L: sätt 1000 ml Buffrad Glukos (25 mg/ml) (83 ml/tim) Om P-Glukos 6-10 mmol/L: sätt 1000 ml Ringer-acetat Om P-Glukos > 10 mmol/L: starta Humulin Reg. inf. (1 E/ml) + 10 % Glukos + (Na+/K+ = 40/20 mmol) enl. algoritm för dosjusteringar Mät P-Glukos varje timme Mål: P-Glukos 6 – 10 mmol/L
 OBS! Under pågående behandling enl. detta PM är all annan ordinerad antidiabetisk. behandling tillfälligt seponerad. ! Sätt alltid 10 % Glukos med (Na+/K+=40/20 mmol) i samband med insulin infusion ! A: KOSTBEHANDLING ELLER PERORALT ANTI-DIABETIKUM. A1: Mindre kirurgi/Dagkirurgi: Fasta 6 tim preop. (2 tim för vatten) Inga perorala antidiabetika < 12 timmar innan Op. P-Glukos vid ankomst. Om P-Glukos < 6 mmol/L: sätt 1000 ml Buffrad Glukos 25 mg/ml (83 ml/tim) Om P-Glukos 6 – 14 mmol/L: sätt 1000 ml Ringer Acetat. Om P-Glukos > 14 mmol/L: Kontakta ansv. anestesiolog för ställningstagande till. om operationen kan uppskjutas eller om insulininfusion + 10 % Glukos + (NA+/K+= 40/20 mmol) ska startas (enl. algoritm) Mät P-Glukos varannan timme tills födointag. A2: Större Kirurgi (inneliggande): P-Glukos kvällen före op. (om > 12 mol/L kontakta anestesiolog 62160) Fasta 6 tim preop. (2 tim för vatten/nutritions dryck) Inga perorala antidiabetika < 12 timmar innan op. P-Glukos kl. 06:00 på op-dagen. Om P-Glukos < 6 mmol/L: sätt 1000 ml Buffrad Glukos (25 mg/ml) (83 ml/tim) Om P-Glukos 6-10 mmol/L: sätt 1000 ml Ringer-acetat. Om P-Glukos > 10 mmol/L: starta Humulin Reg. inf. (1 E/ml) + 10 % Glukos + (Na+/K+ = 40/20 mmol) enl. algoritm för dosjusteringar. Mät P-Glukos varje timme. Mål: P-Glukos 6 – 10 mmol/L.")
20
A1/2 fortsatt…. OBS! Om fasta blir > 6 tim: sätt 1000 ml 10 % Glukos + (Na+/K+= 40/20 mmol) (83ml/tim) Postoperativt på Avd: Om P-glukos > 10 mmol/L: fortsätt Humulin Reg. inf. Mät P-Glukos varannan timme Mål: P-Glukos 6-10 mmol/L Vid första måltiden avslutas Humulin Reg. infusionen och P-Glukos mäts därefter varannan timme tills stabilt (6-10 mmol/L) läge (2-3 mättillfälle)
 läge (2-3 mättillfälle)")
21
B: INSULINBEHANDLING B1: Mindre kirurgi / Dagkirurgi:
Vanligt insulinbehov är 0.6 – 0.8 E/kg/dygn vid normal insulinkänslighet. Relativ insulinresistens kan förväntas de första dagarna efter okomplicerad större kirurgi. B1: Mindre kirurgi / Dagkirurgi: Ordinarie doser långtverkande insulin (glargin/detemir (Lantus/Levemir/Insulatard ) fortsätts Fasta 6 tim preop. (2 tim för vatten) Inget kortverkande eller Mix-Insulin på Op. Morgonen P-Glukos vid ankomst Mät P-Glukos varje 1 timma Mål: P-Glukos mmol/L Om P-Glukos < 6: sätt Buffrad Glukos 25 mg/ml (83 ml/tim) Om P-Glukos 6-10 mmol/L: ingen åtgärd Om P-Glukos 10-14: ge 4 E (= 0.04 ml) Humalog/Novorapid s.c. - sätt 1000 ml Ringer-Acetat (83 ml/tim) Om P-Glukos > 14 mmol/L: Kontakta ansv. anestesiolog för ställningstagande till om operationen ska uppskjutas eller om insulininfusion + 10 % Glukos + (Na+/K+ = 40/20 mmol) ska startas (enl. algoritm) Mät P-Glukos varje ½ -1 timma Mål: P-Glukos 6-10 mmol/L Fortsätts tills vanligt födointag
 fortsätts. Fasta 6 tim preop. (2 tim för vatten) Inget kortverkande eller Mix-Insulin på Op. Morgonen. P-Glukos vid ankomst. Mät P-Glukos varje 1 timma. Mål: P-Glukos mmol/L. Om P-Glukos < 6: sätt Buffrad Glukos 25 mg/ml (83 ml/tim) Om P-Glukos 6-10 mmol/L: ingen åtgärd. Om P-Glukos 10-14: ge 4 E (= 0.04 ml) Humalog/Novorapid s.c. - sätt 1000 ml Ringer-Acetat (83 ml/tim) Om P-Glukos > 14 mmol/L: Kontakta ansv. anestesiolog för ställningstagande till om operationen ska uppskjutas eller om insulininfusion + 10 % Glukos + (Na+/K+ = 40/20 mmol) ska startas (enl. algoritm) Mät P-Glukos varje ½ -1 timma. Mål: P-Glukos 6-10 mmol/L. Fortsätts tills vanligt födointag.")
22
B2: Större Kirurgi (inneliggande):
Ordinarie doser långverkande insulin (glargin/detemir (Lantus /Levemir/ Insulatard) kvällen före operation. Om preop. laxering sätts 1000 ml Glukos 10% + (NA+/K+= 40/20 mmol) samma kväll Inget subcutant insulin på operationsdagens morgon Fasta 6 tim preop. (2 tim för vatten / nutrtionsdryck) P-Glukos kl. 06:00 Sätt 1000 ml Glukos 10% + (NA+/K+= 40/20 mmol) (83 ml/tim) Härefter följs algoritmen avseende insulininfusion Mät P-Glukos varje timme Mål: P-Glukos 6-10 mmol/L Postoperativt på Avd: Insulin- och Glukosinfusion fortsätts tills patienten börjar peroralt intag Mät P-Glukos varje timme till stabilt nivå (5-8 mmol/L) - därefter varannan timme Vid första måltid ges ordinarie dos kortverkande insulin s.c. (Humalog/Novorapid) Humulin Reg. inf. stoppas ½ timme senare. När enteral/parenteral näring startas på avd: Se avdelningens PM Vid postop. överflyttning till IVA: Patienten följer IVA: s protokoll för diabetesbehandling
 kvällen före operation. Om preop. laxering sätts 1000 ml Glukos 10% + (NA+/K+= 40/20 mmol) samma kväll. Inget subcutant insulin på operationsdagens morgon. Fasta 6 tim preop. (2 tim för vatten / nutrtionsdryck) P-Glukos kl. 06:00. Sätt 1000 ml Glukos 10% + (NA+/K+= 40/20 mmol) (83 ml/tim) Härefter följs algoritmen avseende insulininfusion. Mät P-Glukos varje timme. Mål: P-Glukos 6-10 mmol/L. Postoperativt på Avd: Insulin- och Glukosinfusion fortsätts tills patienten börjar peroralt intag. Mät P-Glukos varje timme till stabilt nivå (5-8 mmol/L) - därefter varannan timme. Vid första måltid ges ordinarie dos kortverkande insulin s.c. (Humalog/Novorapid) Humulin Reg. inf. stoppas ½ timme senare. När enteral/parenteral näring startas på avd: Se avdelningens PM. Vid postop. överflyttning till IVA: Patienten följer IVA: s protokoll för diabetesbehandling.")
23
ALGORITM FÖR INSULININFUSION (Humulin Regular 1 E/ml)
P-Glukos mmol/L <6 6-7.9 8-9.9 >20 Insulin START-dos (ml/tim) 0,5 1,0 2.0 3,5 5,0 (kontakt ansv.läkare) 6,5 (kontakt ansv.läkare) Dosjusteringar Om P-glukos vid nästa kontroll är > 10 mmol/L ökas dosen med ytterligare 1ml/tim. När P-glukos närmar sig mmol/L sänkas dosen med 0,1 - 0,5 ml/tim. När P-Glukos ligger stabilt 6-10 mmol/L fortsätts med oförändrad insulintillförsel. Om P-glukos faller snabbt (>50 %) halveras insulindosen och P-glukos kontrolleras 1/2 timme. Om P-glukos är 6 mmol/L avbryts insulininfusionen. Om P-glukos är < 6 mmol/L avbryts insulininfusionen. Ge bolusdos (10 ml) Inj Glukos 300 mg/ml och P-glukos kontrolleras varje 1/2 timme. När P-glukos stiger till > 6 omstartas insulininfusionen med ½ infusions- dosen. När/om patienten påbörjar kolhydrattillförsel (enteralt el. parenteralt) ökas infusionen med 1-3 ml/tim under 1 timme. Därefter återgång till den tidigare dosen.
 0,5. 1, ,5. 5,0 (kontakt ansv.läkare) 6,5 (kontakt ansv.läkare) Dosjusteringar. Om P-glukos vid nästa kontroll är > 10 mmol/L ökas dosen med ytterligare 1ml/tim. När P-glukos närmar sig mmol/L sänkas dosen med 0,1 - 0,5 ml/tim. När P-Glukos ligger stabilt 6-10 mmol/L fortsätts med oförändrad insulintillförsel. Om P-glukos faller snabbt (>50 %) halveras insulindosen och P-glukos kontrolleras 1/2 timme. Om P-glukos är 6 mmol/L avbryts insulininfusionen. Om P-glukos är < 6 mmol/L avbryts insulininfusionen. Ge bolusdos (10 ml) Inj. Glukos 300 mg/ml och P-glukos kontrolleras varje 1/2 timme. När P-glukos stiger till > 6 omstartas insulininfusionen med ½ infusions- dosen. När/om patienten påbörjar kolhydrattillförsel (enteralt el. parenteralt) ökas infusionen med. 1-3 ml/tim under 1 timme. Därefter återgång till den tidigare dosen.")
24
Sätt alltid 1000 ml Glukos 100 mg/ml tillsatt 40 mmol Na+/ 20 mmol K+
Sprutpump: 0.5 ml Humulin Regular 100 E/ml blandas i 49.5 ml NaCl 0.9 % (50ml totalt) OBS !! Sätt alltid 1000 ml Glukos 100 mg/ml tillsatt 40 mmol Na+/ 20 mmol K+ (83 ml/tim) i samband med insulin infusion
 OBS !! Sätt alltid 1000 ml Glukos 100 mg/ml tillsatt 40 mmol Na+/ 20 mmol K+ (83 ml/tim) i samband med insulin infusion.")
25
Alltså…. Kost og/eller Tabl. Beh. Diabetes:
Mindre Dag-Kir: B-glukos < 14 Större inneligg. Kir: B-glukos < 6-10 Insulin Beh. Diabetes: Mindre Dag-Kir: B-glukos < 11 Större inneligg. Kir: B-glukos 6-10 O.Naesh

26
Tack för att ni lyssnade…

Liknande presentationer















 SJUKDOM>")



