Ladda ner presentationen
1
MGUS och smouldering myelom
Cecilie Hveding Blimark Vårdenhetsöverläkare Plasmacellsteamet Hematologen Sahlgrenska Universitetssjukhuset, Gbg

3
Historik Jan Waldenström : ”Essentiell benign hypergammaglobulinemi”

4
3 typer Non IgM-MGUS IgM- MGUS Light-chain MGUS
Olik klinik och överlevnad Rajkumar Mayo Clin Proc 2010 MGUS variants Biclonal gammopathies A biclonal gammopathy is defined as the presence of two different M proteins and occurs in 5–8% of patients with MGUS. Biclonal gammopathy of undetermined significance was noted in 37 (65%) of 57 patients who had a biclonal gammopathy.41 Triclonal gammopathy In a review of the literature by Grosbois et al42, triclonal gammopathies were associated with a malignant immunoproliferative disorder in 16 patients, occurred in non-hematologic diseases in five, and were of undetermined significance in three. Idiopathic Bence Jones proteinuria Patients excreting large amounts of a monoclonal light chain (Bence Jones protein) in the absence of end-organ damage may follow a benign course. Seven patients who excreted more than 1 g/day of Bence Jones protein were followed for 7–36 years: MM developed in two, evolving myeloma in one and AL in one; two patients died of unrelated causes; and one patient has been followed for 36 years without evidence of MM or AL.26 Idiopathic Bence Jones proteinuria represents the light-chain equivalent of MGUS. In the future, the serum free light-chain assay will likely better define this group of monoclonal gammopathies. IgM MGUS IgM MGUS was diagnosed in 213 patients in southeastern Minnesota between 1960 and Lymphoma developed in 17 patients (relative risk [RR] 14.8), WM in six (RR 262), AL in three (RR 16.3), and chronic lymphocytic leukemia in three (RR 5.7).43 The risk was approximately 1.5% per year and continued indefinitely. IgD MGUS The presence of an IgD M protein almost always indicates MM, AL, or plasma-cell leukemia. However, two cases of well-documented MGUS have been reported: one patient had 6 years of follow-up without progression, and one remained stable during 8 years of follow-up.44
 of 57 patients who had a biclonal gammopathy.41. Triclonal gammopathy. In a review of the literature by Grosbois et al42, triclonal gammopathies were associated with a malignant immunoproliferative disorder in 16 patients, occurred in non-hematologic diseases in five, and were of undetermined significance in three. Idiopathic Bence Jones proteinuria. Patients excreting large amounts of a monoclonal light chain (Bence Jones protein) in the absence of end-organ damage may follow a benign course. Seven patients who excreted more than 1 g/day of Bence Jones protein were followed for 7–36 years: MM developed in two, evolving myeloma in one and AL in one; two patients died of unrelated causes; and one patient has been followed for 36 years without evidence of MM or AL.26 Idiopathic Bence Jones proteinuria represents the light-chain equivalent of MGUS. In the future, the serum free light-chain assay will likely better define this group of monoclonal gammopathies. IgM MGUS. IgM MGUS was diagnosed in 213 patients in southeastern Minnesota between 1960 and Lymphoma developed in 17 patients (relative risk [RR] 14.8), WM in six (RR 262), AL in three (RR 16.3), and chronic lymphocytic leukemia in three (RR 5.7).43 The risk was approximately 1.5% per year and continued indefinitely. IgD MGUS. The presence of an IgD M protein almost always indicates MM, AL, or plasma-cell leukemia. However, two cases of well-documented MGUS have been reported: one patient had 6 years of follow-up without progression, and one remained stable during 8 years of follow-up.44.")
5
Figure 1 Monoclonal gammopathies diagnosed at Mayo Clinic during 2003
Figure 1 Monoclonal gammopathies diagnosed at Mayo Clinic during Macro, macroglobulinemia; MGUS, monoclonal gammopathy of undetermined significance; SMM, smoldering multiple myeloma. Robert A. Kyle , S. Vincent Rajkumar Monoclonal gammopathies of undetermined significance Best Practice & Research Clinical Haematology, Volume 18, Issue 4, 2005,

6
MGUS Enbart M-komponent, normal skelettröntgen och normal benmärgsbild
Prevalensen hög (1,5-3% över 50 år,3-5 % över 70 år, upp till 10 % bland 80-åriga Göteborgare) Högre hos svarta Risken att utveckla myelom är kring 1 % per år Risken varierar dock med en faktor 30 10% efter 10 år, 21% efter 20 år och 26% efter 25 år cohort from Olmsted County, Minnesota. Among the 17,398 patients tested, 605 cases of MGUS and 16,793 negative controls were identified. The computerized Mayo Medical Index was used to obtain information on all diagnoses between 1975 and 2006, for a total of 422,663 person-year14 diagnoses, five are known to evolve from MGUS: multiple myeloma, AL amyloidosis, lymphoproliferative disorders, WM, and other unclassified plasma cell proliferative disorders. Hip and vertebral fractures, osteoporosis, and hypercalcemia were all significantly increased with MGUS, even in the absence of progression to multiple myeloma 8.6% of 916 black patients had an M protein, compared with 3.6% of white patients in North Carolina, 3-falt vanligare (4 milj veteraner i USA
 Högre hos svarta. Risken att utveckla myelom är kring 1 % per år. Risken varierar dock med en faktor % efter 10 år, 21% efter 20 år och 26% efter 25 år. cohort from Olmsted County, Minnesota. Among the 17,398 patients tested, 605 cases of MGUS and 16,793 negative controls were identified. The computerized Mayo Medical Index was used to obtain information on all diagnoses between 1975 and 2006, for a total of 422,663 person-year14 diagnoses, five are known to evolve from MGUS: multiple myeloma, AL amyloidosis, lymphoproliferative disorders, WM, and other unclassified plasma cell proliferative disorders. Hip and vertebral fractures, osteoporosis, and hypercalcemia were all significantly increased with MGUS, even in the absence of progression to multiple myeloma. 8.6% of 916 black patients had an M protein, compared with 3.6% of white patients in North Carolina, 3-falt vanligare (4 milj veteraner i USA.")
7
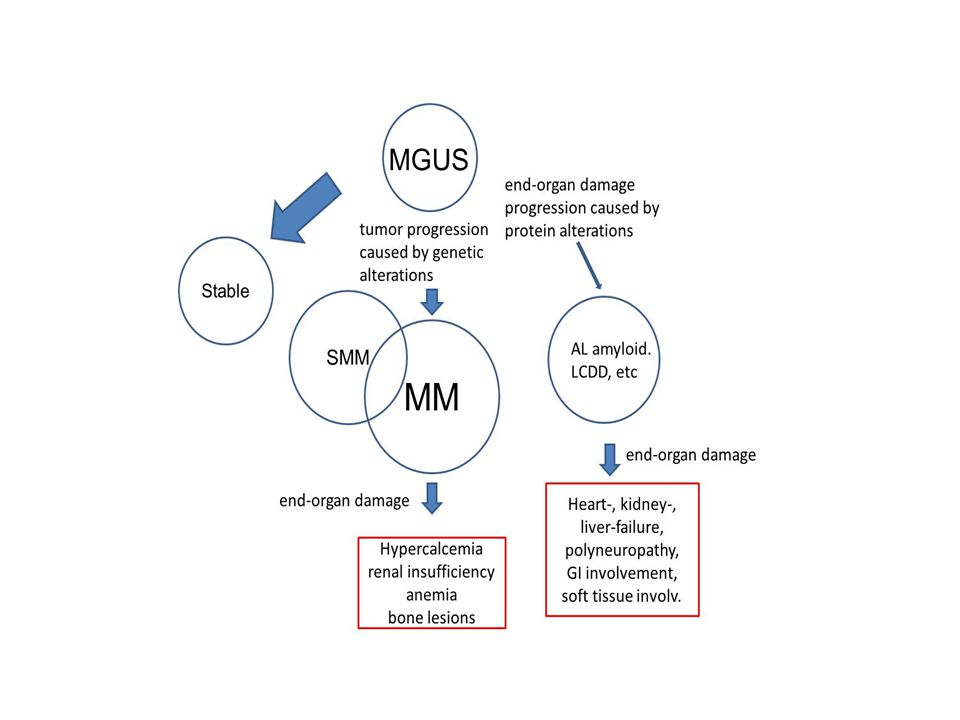
M-component-related diseases.
M-component-related diseases. In B-cell neoplasias (MM indicates multiple myeloma; WM, Waldenström macroglobulinemia; NHL, non-Hodgkin lymphoma; and CLL, chronic lymphocytic leukemia) the clinical pattern is usually dominated by systemic effects caused by expansion of the malignant clone, whereas the monoclonal protein may cause hyperviscosity syndrome or kidney damage. In less common disorders, the biologic effects of the monoclonal protein may account for most of the clinical manifestations and determine the prognosis. There are overlaps between these 2 groups; for instance, the IgM of a patient with Waldenström macroglobulinemia may have a cold agglutinin activity and a myeloma clone can secrete an amyloidogenic light chain. Merlini G , Stone M J Blood 2006;108: ©2006 by American Society of Hematology
 the clinical pattern is usually dominated by systemic effects caused by expansion of the malignant clone, whereas the monoclonal protein may cause hyperviscosity syndrome or kidney damage. In less common disorders, the biologic effects of the monoclonal protein may account for most of the clinical manifestations and determine the prognosis. There are overlaps between these 2 groups; for instance, the IgM of a patient with Waldenström macroglobulinemia may have a cold agglutinin activity and a myeloma clone can secrete an amyloidogenic light chain. Merlini G , Stone M J Blood 2006;108: ©2006 by American Society of Hematology.")
8
MGUS Monoklonal gammopati
B-lymfocytstörning Skall inte ha sympt på myelom benign störning Kan ha hypogammaglobulinemi, hög SR, neuropatier Sekundär MGUS: Reumatologisk Dermatologisk Hepatologiska sjukdomar Neurologisk 25% blir aldri maligna, 50 % hinner dö av andra orsaker, 25 % blir, myelom, waldenström eller lymfom lymphoproliferative disorders, leukemia, other hematologic diseases, connective tissue disorders, neurologic diseases, dermatologic problems, endocrine disorders, liver disease, immunosuppression,

9
Etiologi Vanligare hos släktingar till MGUS o MM
Dvs släktingar har en delad ärftlig eller miljökomponent Insekticider, herbicider o fungicider prevalence of MGUS in first-degree relatives of the MGUS and multiple myeloma probands was 1.9% at ages 40 to 49 years, 6.9% in those 50 to 59 years of age, 11.6% in persons 60 to 69 years of age, 14.6% in those 70 to 79 years old, and 21% in those 80 years of age or older RR hos släkt till MGUS 3.3-falt,RR hos släkt till MM är 2-falt 2-falt risk hos de som arbetar med pesticider

10
Comorbiditet vid MGUS Infektioner Andra
2-faltig risk för infektioner jfr med normalbefolkning Ass. med hypogammaglobulinemi Mer än 3 febrila infektioner pr sesong: empirisk beh med gammaglobuliner Polyneuropati Hudmanifestationer

11
Klinisk bild och laboratoriefynd vid polyneuropathi associerad
till plasmacellsdyscrasi I. MGUS c:a 5 % av MGUS har neuropathi sensorisk eller senso-motorisk, ofta ataxi ingen organförstoring inget hudengagemang inga andra symptom M-komponent IgM > IgG > IgA kappa > lambda M-komponent konc. < 30 g/l BM plasmaceller < 10 % inga skelettlesioner ingen anemi eller trombocytos

12
MGUS-associerad polyneuropathi
I majoriteten av fall med M-komp av typ IgM kan påvisas autoantikropps-aktivitet av M-komp mot komponenter i nervskidan Vanligast är anti MAG ( myelin-associerat glycoprotein ) som kan påvisas med ELISA-teknik Förloppet är oftast ganska godartat och kräver inte annat än understödjande terapi Plasmaferes, intravenöst immunglobulin och steroider har prövats med varierande resultat Rituximab har nyligen i en randomiserad studie visat signifikant effekt. Vid M-komp av typ IgA eller IgG är associationen mellan polyneuropathi vagare och behandlingsrekommendationer ännu mer osäkra.
 som kan påvisas med. ELISA-teknik. Förloppet är oftast ganska godartat och kräver inte annat än understödjande terapi. Plasmaferes, intravenöst immunglobulin och steroider har prövats med. varierande resultat. Rituximab har nyligen i en randomiserad studie visat signifikant effekt. Vid M-komp av typ IgA eller IgG är associationen mellan polyneuropathi. vagare och behandlingsrekommendationer ännu mer osäkra.")
13
Klinisk bild och laboratoriefynd vid polyneuropathi associerad
till plasmacellsdyscrasi II Myelom - förekommer i 1-8 % av MM övervägande sensorisk organförstoring och hudengagemang kan förekomma men är ovanligt skelettsmärtor, trötthet, infektioner M-komponent IgG > IgA kappa > lambda M-komp konc. ofta > 30 g/l BM plasma celler ofta > 10 % lytiska skelettförändringär eller osteoporos anemi vanlig men ej trombocytos

14
Klinisk bild och laboratoriefynd vid polyneuropathi associerad
till plasmacellsdyscrasi Poems ses i 100 % av POEMS övervägande motorisk organomegali och hudengagemang vanligt ödem, trötthet, endokrina abnormiteter IgG > Ig A > IgM nästan alla är lambda M-komp konc i regel < 10g/l BM plasmaceller i regel < 5 % Sklerotiska skelettförändringar i nästan alla fall (undantag Castleman-variant av POEMS) ofta trombocytos
 ofta trombocytos.")
15
Klinisk bild och laboratoriefynd vid polyneuropathi associerad
till plasmacellsdyscrasi IV AL-amyloidos % av AL-amyloidos har polyneuropathi sensorisk och senso-motorisk organförstoring rel vanligt (lever, mjälte) hudförändringar rel. ovanligt trötthet, ödem, cardiomyopathi, nefros IgG > IgA > IgM kappa > lambda M-komp konc vanligen < 20 g/l BM plasmaceller < 10 % inga skelettförändringar trombocytos förekommer, anemi sällan
 hudförändringar rel. ovanligt. trötthet, ödem, cardiomyopathi, nefros. IgG > IgA > IgM kappa > lambda. M-komp konc vanligen < 20 g/l. BM plasmaceller < 10 % inga skelettförändringar. trombocytos förekommer, anemi sällan.")
16
Klinisk bild och laboratoriefynd vid polyneuropathi associerad
till plasmacellsdyscrasi V. Cryoglobulinemi förekommer hos c:a 25 % dominerande sensorisk organförstoring är ovanligt purpura, arthralgier, hepatit, nefrit IgM >> IgG > IgA kappa > lambda M-komp konc. i regel < 20 /l BM plasmaceller ofta < 5 % inga skelettföändringar ofta anemi, sällan trombocytos

17
MGUS sek till andra sjukdomar
Hematologiska sjd Andra KLL DLCL HCL (KML,AML) vWillebrand (acquired) Mb Waldenstöm RA Lupus Ankyliserande Spondylit Polymyositis Sclerodermi Lichen myxedömatosis Pyoderma gangrenosum Schnitlers syndrom Hepatit (C) Transplanterade (immunosuppression)
 vWillebrand (acquired) Mb Waldenstöm. RA. Lupus. Ankyliserande Spondylit. Polymyositis. Sclerodermi. Lichen myxedömatosis. Pyoderma gangrenosum. Schnitlers syndrom. Hepatit (C) Transplanterade. (immunosuppression)")
18
Hudsjukdomar associerade med monoklonal gammapathi
Scleromyxödem Schnitzlers syndrom Pyoderma gangrenosum Xanthomatos

19
Scleromyxödem Dermal deponering av mucin och kollagen
Symmetrisk utsådd av 2-3 mm stora vaxliknande papler som utvecklas till större sammanhängande indurationer, sclero- dactyli och minskar rörlighet. Förändringarna kan drabba även andra organ. Mer än 80 % har M-komp av typ IgG. Den är oftast lambda och katodal vid elektrofores Patogenes oklar, möjligen autoantikroppsaktivitet Behandling riktad mot plasmacellsdyskrasin inklusive HDM/ASCT kan ge remissioner

20
Schnitzlers syndrom Kronisk eller recidiverande urticariell rodnad
Periodisk feber Arthralgier, bensmärtor M-komponent nästan alltid IgG och dominerande kappa, Patogenesen oklar. Autoantikropp? Behandling med Anakrina – en syntetisk analog av endogen IL-1-receptor antagonist ger remission i hög frekvens men recidiv är vanliga

21
Pyoderma gangrenosum. En ovanlig kronisk ulcerös hudsjukdom med stora nekrotiska sår fr. a. på benen Associerad med bakomliggande sjukdomar som inflammatorisk tarmsjukdom och rheumatisk sjukdom samt monoklonal gammapathi Av 67 patienter diagnosticerade på Mayo-kliniken under 12 år hade 8 (12 %) monoklonal gammapathi, nästan alltid IgA Patogenesen är ej klarlagd
 monoklonal gammapathi, nästan alltid IgA. Patogenesen är ej klarlagd.")
22
Nekrobiotisk xanthogranulomatos
Sällsynt sjukdom med xanthogranulomatösa plaques längs orbitakanterna Monoklonal gammapathi av IgG-typ rapporterad i upp till 73 % i en serie. Makrofagerna i lesionen innehåller apolipoproteinB och M-komponent i ett komplex

23
Konklusioner. Små monoklonala plasmacellsproliferationer som tumörbiologiskt uppträder som MGUS kan vara patogena p.g.a. biologisk aktivitet av M-komponenten Tillstånden är ovanliga, med ett smygande insjuknande och de kliniska manifestationerna varierande varför diagnosen ofta förbises Patienterna har ofta varit på en odysse hos olika specialister – nefrologer, kardiologer, rheumatologer, gastroenterologer - innan diagnosen ställs Fyndet av en M-komponent kan vara signalen som klarlägger bilden. Tidig diagnos och adekvat behandling kan i många fall förhindra eller förbättra organskada , förbättra livskvalitet och förlänga överlevnad. Även små M-komponenter skall rapporteras och fyndet ställas i relation till patientens samlade symptombild

24
Biology of myelomagenesis.
Biology of myelomagenesis. Progression from a normal postgerminal center B cell to symptomatic myeloma involves a series of genetic and phenotypic changes. Early genetic events can be categorized into 2 major types, hyperdiploid type and nonhyperdiploid type. These are unified by cyclin D dysregulation (30). The role of 13q seems to be less certain and it may be an early or late event. Secondary genetic changes include Ras mutations, NF-κB pathway–activating mutations, and inactivating mutations of p53, PTEN, or RB pathways (1). Several other genetic changes also occur along the way, including secondary translocations, increase in copy number abnormalities, HOXA9 overexpression, and Myc upregulation (21, 36). The end result of these changes includes a clonal expansion of abnormal plasma cells that occupy bone marrow stem cell niches (45). Lytic bone lesions are seen due to increased osteoclast activation resulting from RANK-L signaling and osteoblast inhibition from DKK1 activity (41, 44). Immune evasion, paracrine, and autocrine signaling mediated by cytokine and growth factors are important final steps (46, 51). Agarwal A , and Ghobrial I M Clin Cancer Res 2013;19: ©2013 by American Association for Cancer Research
. The role of 13q seems to be less certain and it may be an early or late event. Secondary genetic changes include Ras mutations, NF-κB pathway–activating mutations, and inactivating mutations of p53, PTEN, or RB pathways (1). Several other genetic changes also occur along the way, including secondary translocations, increase in copy number abnormalities, HOXA9 overexpression, and Myc upregulation (21, 36). The end result of these changes includes a clonal expansion of abnormal plasma cells that occupy bone marrow stem cell niches (45). Lytic bone lesions are seen due to increased osteoclast activation resulting from RANK-L signaling and osteoblast inhibition from DKK1 activity (41, 44). Immune evasion, paracrine, and autocrine signaling mediated by cytokine and growth factors are important final steps (46, 51). Agarwal A , and Ghobrial I M Clin Cancer Res 2013;19: ©2013 by American Association for Cancer Research.")
25
Biological events related to progression to multiple myeloma.
Biological events related to progression to multiple myeloma. The biologic transition from normal plasma cells to multiple myeloma precursor disease (monoclonal gammopathy of undetermined significance [MGUS] and smoldering myeloma) to multiple myeloma consists of many overlapping oncogenic events. These events do not all occur in each affected individual, for example, hyperdiploidy is present in approximately 50% of precursor and multiple myeloma tumors. In this illustration, solid lines approximate the period during which the oncogenic event is likely to occur; dashed lines indicate less certainty in the timing. Once an oncogenic event occurs, it almost always persists. The 2 major types of early events include IgH translocations [most commonly: t(4;14), t(14;16), t(6;14), t(11;14), and t(14;20)] and hyperdiploidy, although most tumor cells have only one of these two events. Either of these can coexist with deletion of chromosome 13, although this abnormality most commonly (> 80% to 90% of patients) occurs with the t(4;14), t(14;16), and t(14;20) IgH translocations.38,39 A unifying early event in most, perhaps all, precursor and multiple myeloma tumors is the dysregulation of a cyclin D gene. Secondary translocations, sometimes involving an Ig locus, can occur at any stage of myelomagenesis. Activating mutations of NRAS and KRAS are each present in about 15% of multiple myeloma tumors; NRAS mutations are present in MGUS tumors and KRAS mutations are absent from MGUS tumors. Constitutive activation of the nuclear factor κB (NFκB) pathway is mediated by mutations in some tumors during progression.38 Other events, such as Rb gene inactivation or deletion of p53 or p18 genes, are mostly seen at the level of advanced intramedullary or extramedullary multiple myeloma.38,65 Through the stage of intramedullary multiple myeloma, the tumor cells are strongly dependent on the bone marrow microenvironment.66 The reciprocal interaction of the bone marrow microenvironment and the tumor cells results in changes in the bone marrow microenvironment, which are responsible for the lytic lesions that are characteristic of multiple myeloma. Extramedullary tumor cells have developed features that make them independent of the bone marrow microenvironment. (Reprinted with permission.37) Korde N et al. Blood 2011;117: ©2011 by American Society of Hematology
 to multiple myeloma consists of many overlapping oncogenic events. These events do not all occur in each affected individual, for example, hyperdiploidy is present in approximately 50% of precursor and multiple myeloma tumors. In this illustration, solid lines approximate the period during which the oncogenic event is likely to occur; dashed lines indicate less certainty in the timing. Once an oncogenic event occurs, it almost always persists. The 2 major types of early events include IgH translocations [most commonly: t(4;14), t(14;16), t(6;14), t(11;14), and t(14;20)] and hyperdiploidy, although most tumor cells have only one of these two events. Either of these can coexist with deletion of chromosome 13, although this abnormality most commonly (> 80% to 90% of patients) occurs with the t(4;14), t(14;16), and t(14;20) IgH translocations.38,39 A unifying early event in most, perhaps all, precursor and multiple myeloma tumors is the dysregulation of a cyclin D gene. Secondary translocations, sometimes involving an Ig locus, can occur at any stage of myelomagenesis. Activating mutations of NRAS and KRAS are each present in about 15% of multiple myeloma tumors; NRAS mutations are present in MGUS tumors and KRAS mutations are absent from MGUS tumors. Constitutive activation of the nuclear factor κB (NFκB) pathway is mediated by mutations in some tumors during progression.38 Other events, such as Rb gene inactivation or deletion of p53 or p18 genes, are mostly seen at the level of advanced intramedullary or extramedullary multiple myeloma.38,65 Through the stage of intramedullary multiple myeloma, the tumor cells are strongly dependent on the bone marrow microenvironment.66 The reciprocal interaction of the bone marrow microenvironment and the tumor cells results in changes in the bone marrow microenvironment, which are responsible for the lytic lesions that are characteristic of multiple myeloma. Extramedullary tumor cells have developed features that make them independent of the bone marrow microenvironment. (Reprinted with permission.37) Korde N et al. Blood 2011;117: ©2011 by American Society of Hematology.")
26
Progression till MM Orsaker oklara Genetisk
BM angiogenes (median microvessel density) Cytokiner rel till MM skelettsjukdom (RANKL OPG) Riskfaktorer: Icke IgG, M-komp>15, FLC-kvot patologisk Of patients with multiple myeloma, 60% have an immunoglobulin H (IgH) (14q32) translocation with fluorescence in situ hybridization (FISH) [24]. In one series, IgH translocations were found in 27 (46%) of 59 patients with MGUS [25]. In another report, translocations consisting of t(11;14)(q13;q32) were found in 25%, t(4;14)(p16.3;q32) in 9%, and t(14;16)(q32;q23) in 5% [26]. These translocations lead to the dysregulation of oncogenes such as cyclin D, c-MAF, FGFR3-MMSET, and cyclin D3; they may play a role in the initiation of the MGUS clone rather than in the progression of MGUS to multiple myeloma. In another report, Chng et al. [27] reported that 40% of 28 patients with SMM or MGUS had hyperdiploidy. Deletions of chromosome 13 are found in similar frequencies in both multiple myeloma and mm BM Angiogenesmedian microvessel density was 1.3 in normal controls, 1.7 in AL amyloidosis, 3 in MGUS, 4 in SMM, 11 in multiple myeloma, and 20 in relapsed multiple myeloma nuclear factor kappa B ligand (RANKL) and macrophage inhibitory protein 1 α (MIP1α) play an important role in the development of bone lesions. Osteoprotegerin (OPG) modulates RANKL. The excess RANKL or reduced levels of OPG may produce myeloma bone disease. Interleukin-1β also has strong osteoclast-activating factor activity. Interleukin-6 (IL-6) and tumor necrosis factor-α may also play a role.
 Cytokiner rel till MM skelettsjukdom. (RANKL OPG) Riskfaktorer: Icke IgG, M-komp>15, FLC-kvot patologisk. Of patients with multiple myeloma, 60% have an immunoglobulin H (IgH) (14q32) translocation with fluorescence in situ hybridization (FISH) [24]. In one series, IgH translocations were found in 27 (46%) of 59 patients with MGUS [25]. In another report, translocations consisting of t(11;14)(q13;q32) were found in 25%, t(4;14)(p16.3;q32) in 9%, and t(14;16)(q32;q23) in 5% [26]. These translocations lead to the dysregulation of oncogenes such as cyclin D, c-MAF, FGFR3-MMSET, and cyclin D3; they may play a role in the initiation of the MGUS clone rather than in the progression of MGUS to multiple myeloma. In another report, Chng et al. [27] reported that 40% of 28 patients with SMM or MGUS had hyperdiploidy. Deletions of chromosome 13 are found in similar frequencies in both multiple myeloma and mm. BM Angiogenesmedian microvessel density was 1.3 in normal controls, 1.7 in AL amyloidosis, 3 in MGUS, 4 in SMM, 11 in multiple myeloma, and 20 in relapsed multiple myeloma. nuclear factor kappa B ligand (RANKL) and macrophage inhibitory protein 1 α (MIP1α) play an important role in the development of bone lesions. Osteoprotegerin (OPG) modulates RANKL. The excess RANKL or reduced levels of OPG may produce myeloma bone disease. Interleukin-1β also has strong osteoclast-activating factor activity. Interleukin-6 (IL-6) and tumor necrosis factor-α may also play a role.")
27
Riskfaktorer för progress MGUS
Rajkumar Blood, 2005

28
Risk-stratifieringsmodell
för MGUS IMWG Kyle Leukemia 2010

29
Handläggning MGUSSvenska Riktlinjer Pl.cellssjd 2013
Hög ålder o låg M-komponent (<5g/l) Ingen uppföljning <15g/l 3-4 ggr pr år 1a året sedan 1x/år (Primärvård) >15g/L 3-4 ggr pr år 1a året sedan 1x/år (Int.med/hema) Oftare om: IgM>10 g, IgD, IgE oavsett konc Bence-Jones, krea stigande Patienten är sin bästa kontroll, information! TnT o NT pro Bnb bör kontroleras ngn gång i början sp att man inte missar en AL-Amyyloidos under uppsegling.
 Ingen uppföljning. <15g/l 3-4 ggr pr år 1a året sedan 1x/år (Primärvård) >15g/L 3-4 ggr pr år 1a året sedan 1x/år (Int.med/hema) Oftare om: IgM>10 g, IgD, IgE oavsett konc. Bence-Jones, krea stigande. Patienten är sin bästa kontroll, information! TnT o NT pro Bnb bör kontroleras ngn gång i början sp att man inte missar en AL-Amyyloidos under uppsegling.")
30
Smouldering myelom (asymtomatisk)
12-17% av alla nydiagnosticerade MM 3-årsöverlevnad på svenska patienter 81% Risk att gå över i symptomatisk plasmacellssjukdom är 10% per år första 5 åren, 3% per år nästa 5 år och därefter likt MGUS med 1-2% risk per år The risk of smoldering (asymptomatic) multiple myeloma (SMM) progressing to multiple myeloma or a related disorder is 10% per year for the first 5 years, 3% per year for the next 5 years and 1–2% per year for the next 10 years
 multiple myeloma. (SMM) progressing to multiple myeloma or a related disorder is. 10% per year for the first 5 years, 3% per year for the next. 5 years and 1–2% per year for the next 10 years.")
31
Diagnoskriterier The International Working Group 2003
Asymptomatisk myelom M-komponent i s. >30g/l och/eller Plasmaceller i benmärg >10% Inga myelomrelaterade organskador Symptomatisk myelom M-komponent Plasmaceller i benmärg eller plasmacellstumor Myelomrelaterad organ-eller vävnadsskada =behandlingskrävande

32
Smouldering MM FAKTORER SOM GER ÖKAD RISK FÖR PROGRESSION FLC -kvot<0.125 och > 8 är oberoende risk faktor för progress till sympt MM Pl.celler >10% + > 30 g/l i benmärgen = HÖGRISK- SMM 10, 5.1 och 1.9 år till progression om man har 0 en eller båda riskfaktorer The cumulative probability of progression at 15 years was 87% for the 106 patients in group 1 (≥10% plasma cells and ≥3 g of monoclonal protein per deciliter), 70% for the 142 patients in group 2 (≥10% plasma cells and <3 g of monoclonal protein per deciliter), and 39% for the 27 patients in group 3 (<10% plasma cells and ≥3 g of monoclonal protein per deciliter) progression”), recent studies suggest that additional features such as BM plasmacytosis 60%48; an abnormal FLC-ratio 100 (involved kappa) or (involved lambda)39; and/or focal BM lesions detected by functional imaging including PET-CT and/or MRI47,49 in asymptomatic individuals may warrant a clinical diagnosis of multiple myeloma. FIGURE 3 Probability of Progression to Active Multiple Myeloma or Primary Amyloidosis in Patients with Smoldering Multiple Myeloma among Three Risk Groups. ). The median time to progression was 2 years in group 1, 8 years in group 2, and 19 years in group 3 (P<0.001). Dispenzieri Blood
, 70% for the 142 patients in group 2 (≥10% plasma cells and <3 g of monoclonal protein per deciliter), and 39% for the 27 patients in group 3 (<10% plasma cells and ≥3 g of monoclonal protein per deciliter) progression ), recent studies suggest that additional features such as BM. plasmacytosis 60%48; an abnormal FLC-ratio 100 (involved. kappa) or 0.01 (involved lambda)39; and/or focal BM lesions. detected by functional imaging including PET-CT and/or MRI47,49. in asymptomatic individuals may warrant a clinical diagnosis of. multiple myeloma. FIGURE 3. Probability of Progression to Active Multiple Myeloma or Primary Amyloidosis in Patients with Smoldering Multiple Myeloma among Three Risk Groups. ). The median time to progression was 2 years in group 1, 8 years in group 2, and 19 years in group 3 (P<0.001). Dispenzieri Blood.")
33
The risk of smoldering (asymptomatic) multiple myelom(SMM) progressing to multiple myeloma or a related disorder is 10% per year for the first 5 years, 3% per year for the next 5 years and 1–2% per year for the next 10 years

34
Hög-risk SMM i Sverige Av alla patienter med >10% pl.celler OCH >30g/l i M-komponent 56% hade progredierat vid 2 år Kristinsson NEJM 2013

35
Nya riskfaktorer >60% pl.celler i BM (ultra-highrisk)
FLC-kvot>100 (kappa) eller <0.01(lambda) 2 eller fler fokala läsioner vid MRI Rajkumar. N Engl J Med. 2011 Larsen JT,. Leukemia. 2013 Hillengass J,.J Clin Oncol. 2010
 eller <0.01(lambda) 2 eller fler fokala läsioner vid MRI. Rajkumar. N Engl J Med Larsen JT,. Leukemia Hillengass J,.J Clin Oncol")
38
Original Article Lenalidomide plus Dexamethasone for High-Risk Smoldering Multiple Myeloma
María-Victoria Mateos, M.D., Ph.D., Miguel-Teodoro Hernández, M.D., Pilar Giraldo, M.D., Javier de la Rubia, M.D., Felipe de Arriba, M.D., Ph.D., Lucía López Corral, M.D., Ph.D., Laura Rosiñol, M.D., Ph.D., Bruno Paiva, Ph.D., Luis Palomera, M.D., Ph.D., Joan Bargay, M.D., Albert Oriol, M.D., Felipe Prosper, M.D., Ph.D., Javier López, M.D., Ph.D., Eduardo Olavarría, M.D., Ph.D., Nuria Quintana, M.D., José-Luis García, M.D., Joan Bladé, M.D., Ph.D., Juan-José Lahuerta, M.D., Ph.D., and Jesús-F. San Miguel, M.D., Ph.D. N Engl J Med Volume 369(5): August 1, 2013
: August 1,")
39
Randomization and Follow-up of the Patients Included in the Trial.
Figure 1 Randomization and Follow-up of the Patients Included in the Trial. A total of 125 patients underwent randomization (6 patients were excluded because they did not meet the criteria of smoldering multiple myeloma at high risk for progression); 57 patients were assigned to treatment with lenalidomide and dexamethasone, and 62 were assigned to observation. Mateos M-V et al. N Engl J Med 2013;369:
; 57 patients were assigned to treatment with lenalidomide and dexamethasone, and 62 were assigned to observation. Mateos M-V et al. N Engl J Med 2013;369:")
40
Survival Outcomes in the Per-Protocol Population.
Figure 2 Survival Outcomes in the Per-Protocol Population. Panel A shows the Kaplan–Meier estimates of time to progression to symptomatic disease. Panel B shows overall survival from the date of inclusion in the study. Panel C shows overall survival from the date of diagnosis of smoldering multiple myeloma. Mateos M-V et al. N Engl J Med 2013;369:

41
Best Responses during the Induction and Maintenance Phases in the Treatment Group, According to the Per-Protocol Analysis. Table 2 Best Responses during the Induction and Maintenance Phases in the Treatment Group, According to the Per-Protocol Analysis. Mateos M-V et al. N Engl J Med 2013;369:

42
Adverse Events of Clinical Interest in the Safety Population, According to Grade.
Table 3 Adverse Events of Clinical Interest in the Safety Population, According to Grade. Mateos M-V et al. N Engl J Med 2013;369:

43
Conclusions Early treatment for patients with high-risk smoldering myeloma delays progression to active disease and increases overall survival.

44
Uppföljning o diagnostik IMWG 2010
the 2010 IMWG guidelines state that in SMM patients, an SPEP and physician visit should be repeated every 2 to 3 months for first year, followed by every 4 to 6 months for 1 year, with eventual 6- to 12-month evaluations if clinically stable thereafter.6 In SMM, beyond mandatory baseline BM examination and skeletal survey, the guidelines recommend magnetic resonance imaging (MRI) of the spine and pelvis because it can detect occult lesions, which, if present, predict for a more rapid progression to multiple myeloma.6,47 It is critical to recognize that in a disease such as multiple myeloma
 of the spine and pelvis because. it can detect occult lesions, which, if present, predict for a more. rapid progression to multiple myeloma.6,47. It is critical to recognize that in a disease such as multiple myeloma.")














 hos kvinnor>")
 hos kvinnor>")





