Ladda ner presentationen
Presentation laddar. Vänta.

1
Hur arbetar Finland preventivt med sexuell hälsa? Hur lyckas man så bra?? Dan Apter dan.apter@vaestoliitto.fi Kliniken för sexuell hälsa Väestöliitto Sexual Health Clinic

2
Lyckas man bra ? Varför lyckas man inte bättre ?

3
Dan Apter Överläkare vid Klinken för sexuall hälsa, Väestöliitto Specialist i gynekologi och obstetrik, docent Grundare och ordförande för Barn- och ungdomsgynekologiska föreningen i Finland, 1994- 2009 Ordförande för Sexologiska föreningen i Finland 2003-05 Ordförande, International Federation of Pediatric and Adolescent Gynecology, 2001-2007 European Society of Contraception and Reproductive Health, viceordförande 2008-

4
Sweden has the highest abortion rate in Europe, with the exception of some Eastern European countries, why?

5
Do we have information? Background for differences?? Available data about sexual and reproductive health (SRH) of adolescents and children in the various Nordic countries: abortion and delivery rates, STI, contraceptive use, sexual behavior, sexual abuse, other health aspects, gender equality, happiness and quality of life? ? Present ways SRH services of adolescents are provided Education of professionals in relation to SRH of adolescents and children
 of adolescents and children in the various Nordic countries: abortion and delivery rates, STI, contraceptive use, sexual behavior, sexual abuse, other health aspects, gender equality, happiness and quality of life. Present ways SRH services of adolescents are provided Education of professionals in relation to SRH of adolescents and children.")
6
SEXUAL HEALTH FOR ADOLESCENTS 1.Recognizing sexual rights 2.Sexuality education and counselling 3.Confidential high quality services

7
Finland 60 years ago There was poor country, suffering the consequences of war STIs were common Contraception hardly existing, Women dying of illegal abortion

8
Changing attitudes During the 1960s a new culture revolved, with freedom for teenagers including sexual behavior Adolescent childbirths peaked in the late 1960s in northern and western Europe With liberalization of legislation, increasing numbers opted for abortion in the 70s In some countries, adolescent premarital sex was mainly approached from a moral point of view; the Scandinavian countries were primarily concerned with health consequences

9
Changing attitudes The Scandinavian approach was to create preconditions for safer sex: increase sexuality education, availability of contraceptive methods, and accessibility to sexual health services Balance between prevention of pregnancies, prevention of STIs, allowing for sexuality as a positive resource rather than a threat

10
Background for changes The Nordic experience shows, that with persistent and committed actions many problems can be prevented and solved. Requires political commitment

11
Sexual/reproductive health Today sexual health is relatively good in the Nordic countries according to available indicators: Maternal and perinatal mortality is very low Incidence of abortions rather low Incidence of HIV very low Teenage pregnancy rare Gender equality good

12
Legislation in Finland The abortion law 1970, contraceptive counseling obligatory The Public Health Law (1972) guarantied free primary health care including contraceptive services for the whole population Sexuality education was integrated into school programs in 1970 to ensure practice of safer sex.
 guarantied free primary health care including contraceptive services for the whole population Sexuality education was integrated into school programs in 1970 to ensure practice of safer sex.")
13
Responsibility of municipalities in Finland Contraceptive counseling units were founded throughout the country. Public health nurses & midwifes well trained School health developed, school health nurses participated in sexuality education Close connection between education and services

14
Legal abortion per 1000 15-49 yr in the Nordic countries Finland Sweden

15
Deliveries in 15-19 yr olds in the Nordic countries

16
Abortions in 15-19 yr olds in the Nordic countries

17
Induced abortions in nordic countries per thousand women aged 15-49 in 2007

18
Antalet aborter och förlossningar per 1000 flickor 15-19 år

19
1 oktober 2015 L Marions19

20
Attityder till abort i Sverige och Finland http://www.worldvaluessurvey.org/

21
1995: ”The Evolution of Sexual Health in Finland: How we did it” 2000: ”The Evolution of Sexual Health in Finland: How we spoiled it” 2010: How we did it again?

22
Abortions and deliveries per 1000 girls 15-19 year old in Finland 1975 to 1995

23
Factors affecting sexual health in mid 90 th in Finland Economical depression, services cut School health services cut Sexuality education in schools became an optional subject in 1994, now obligatory again Population responsibility led to the close down of contraceptive counseling centers The local municipalities implement health care policy independently, even without necessary qualifications

24
Abortions and deliveries (per 1000) in 15-19 yr old girls in Finland 1975 - 2008 8,8
 in yr old girls in Finland ,8")
25
Preventivmetod vid senaste samlag, och % andel flickor som haft samlag STAKES, 2008 GrundskolaGymnasiumYrkesskola 8. årskurs 9. årskurs 1. årskurs 2. årskurs 1. årskurs 2. årskurs Ingenting201577 13 Kondom6153 443630 P-piller112331394047 Kondom och p-piller 688978 Haft samlag, % av alla143036526979

26
% girls who have had intercourse, Finland 1996-2007 STAKES school health survey

27
%-girls who did not use contraception at last intercourse

28
Sexually transmitted infections STIs were common when our parents/ grandparents were young, gc 24 000/yr in the mid 40th Were common when we/our parents were young, gc 15 000/yr in mid 70th And they are common again, chlamydia 14 000/yr

29
Chlamydia, Number of reported cases in Norway 6,0 % of tests + in 2000 7,7 % of tests + in 2006

30
Clamydia in the Nordic countries 2002-2008

31
Number of reported chlamydia cases Reporting system changed in 1995 KTL

32
Reported number of STI:s in Finland KTL Chlamydia reprting system changed in 1995

33
Reported number of chlamydia cases by age in 2005

34
Reported numbers of chlamydia among 15-19 year old girls and boys in Finland 1988-2009 per 10 000

35
Chlamydia testing patterns Bakken et al, Sexually Transmitted Diseases 33:26-30, 2006 Chlamydia testing patterns, prevalence, in central Norway 1990-2003 4% of men and 44% of women had undergone chlamydia testing at least once by the age 20; 44% respectively 84% by age 25.

36
Regler om könssjukdomar, Finland Undersökning och behandling av könssjukdomar är i princip kostnadsfria för patienten inom den offentliga sektorn Smittospårning fungerar varierande Klamydia rapportering enbart från laboratorier Gc, syfilis och HIV rapporteras också av läkare Papa screening har fungerat bra, cx ca insidensen lägst

37
Vad görs i Finland Alla inklusive ungdomar betalar fullt pris för kondomer De senaste 10 åren minimal kampanjaktivitet Rekommendation 2007: Klamydiaprov tas av alla nya preventivmedelsklienter under 25 år vid första besök eller 3 månaders uppföljning, samt vid ett års uppföljning. (men få känner till denna rekommendation, och ännu färre följer den)
.")
38
Karakteristiska för klamydiasmitta, 23 487 klamydiapatienter som behandlats vid poliklinikerna för könssjukdomar 1995-2006 Men %Kvinnor % Smittad i Finland92,795,3 Besmittad av tillfällig sexpartner4935 Möjligt att klamydia förts vidare3534 Haft klamydia inom det senaste året1316 Tid från smitta till diagnos30 (16-58)40 (20-81)
40 (20-81)")
39
Klamydia prevalens Vid HPV vaccinering fas III studier togs klamydiaprov av 5000 flickor, 16-17 år gamla 2004-2005, 2,5% klamydia +.

40
HPV Infection Occurs Shortly after Sexual Debut Collins et al: Br J Obstet Gynecol 2002;109: 96 Time since first intercourse (months)
")
41
Sex and HIV Education Programs: Their Impact on Sexual Behaviors of Young People Throughout the World Douglas B. Kirby, B.A. Laris, Lori A. Rolleri Journal of Adolescent Health 2007, 40: 206–217 reviewed 83 studies that measured the impact of curriculum- based sexuality education programs on sexual behavior and mediating factors < 25 years anywhere in the world.

42
Sexuality education works ! Two thirds of the programs significantly improved one or more sexual behaviors. The evidence is strong that programs do not hasten or increase sexual behavior but, instead, some programs delay or decrease sexual behaviors or increase condom or contraceptive use. Programs were effective across a wide variety of countries, cultures, and groups of youth. Replications of studies also indicate that programs remain effective when implemented by others in different communities, provided all the activities are implemented as intended in similar settings.

43
Impact on contraceptive use Condom use Of the 54 studies measuring program impact on condom use, almost half (48%) showed increased condom use; none found decreased condom use.
 showed increased condom use; none found decreased condom use.")
44
Sexual abstinence only programmes to prevent HIV infection in high income countries: systemic review Underhill et al BMJ 2007 13 trials enrolling 16 000 US youths identified, all outcomes were self reported No program affected incidence of unprotected sex, number of partners, condom use, or sexual initiation

45
How good is the evidence for effect of sex education on different outcomes? Judith Stephenson Margaret Pyke Professor of Sexual & Reproductive Health, UK

46
Sexuality education as part of health teaching Sexual health: human relations, sexuality, behavior, values and norms The student should learn basics of sexual health, the importance of contraception and methods for it, and be able to consider and justify responsible sexual behavior The student should be able to name, recognize and reveal different feelings, and describe their development and reasons, and provide examples how behavior and interactions can be regulated according to the situation Ministry of education, guidelines for teaching 2004, but my translation

47
Aim and structure of the sexual health knowledge study Produce a representative picture of sexuality education of school grade 7-9 in 2006, and the changes from 1996, particularly related to the introduction of a new subject, health, as described by teachers Evaluate the sexual health knowledge of 8 grade students by a national quiz, and changes between 2000 and 2006 Combine the information provided by the teachers with knowledge of the students in the same schools, to evaluate the impact of sexuality education Väestöliitto 2007

48
A study of students’ sexual health knowledge Carried out in 2000 and 2006 in the form of a quiz at grade 8. In 2000 number of participating students was 30241 from 401 schools In 2006 number of participating students was 33819 from 462 schools

49
Lärarna Varierande bakgrund, men fått specialutbildning Mer varierande metoder används Endast 4% tyckte att det var svårt att tala om sexualitet, 80% tyckte att det var lätt En lärare i skolan ansvarig för planering och koordinering, enligt curriculum

50
Mean hours of sexuality education per grade in 1996 and 2006 in Finland Grade 7Grade 8Grade 9 19962,54,37,9 20065,98,76,2 Väestöliitto 2007

51
A study of students’ sexual health knowledge 75 questions in common in 2000 and 2006 In 2000, mean number of correct answers was 49,6 and 51,5 in 2006 The number of correct answers increased for girls from 53,9 to 55,1, and for boys from 45,4 to 48,3

52
Q41. Emerency contraception should be used: 1.in a week from unprotected intercource 2.in two weeks from the absence of periods 3.as soon as possible, but at the latest 72 hours from unprotected intercource 4.at the latest six hours from unprotected intercource

53
Effect of sexuality education and school performance on sexual health knowledge school performance several lessons one lesson no lessons no health educ. Together 8,5-1054,849,150,339,952,9 7,5-8,451,947,147,642,950,3 6,5-7,448,343,245,539,746,8 <6,545,040,339,837,342,8 Together51,145,647,240,449,3 sexuality educ in health Väestöliitto 2007

54
Sexual health services Services for adolescents can be provided in various settings. The clinic should have a youth-friendly atmosphere, where young people can feel welcome and comfortable. Unquestionable confidentiality is important. The providers must not moralize and judge the adolescents, but treat adolescents with respect indicating that young people are important.

55
Services for adolescents contraception, STI treatment, counseling and testing for HIV pregnancy care and post abortion management; management of sexual violence; mental health services, including services to address the use of tobacco, alcohol and drugs; information and counseling on development during adolescence, including nutrition, hygiene, sexuality The appropriate range of essential services must be decided based on local needs assessments.

56
Median age of first intercourse, Finland Girls 16,8 yr Boys 17,4 yr Based on 200 000 answers of 13-19 yr olds to a questionnaire in 2008-09 Simopekka Vänskä, THL

57
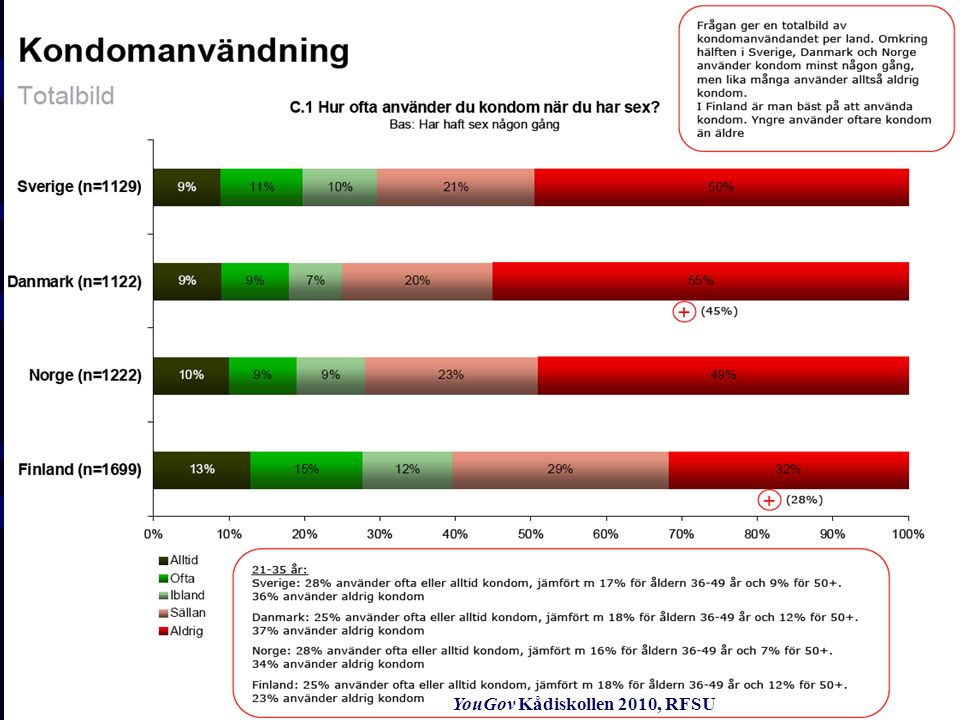
Kådiskollen 2010, RFSU –YouGovs Internetpanel bestående av 46 000 förrekryterade kvinnor och män i åldrarna 15- 74 år som vill delta i undersökningar. –Dessa utgör ett representativt urval av befolkningen vad gäller kön, ålder och region. Målgruppen är personer som minst någon gång haft sex. –Målgrupp Sverige: 1129, Danmark: 1122, Norge:1222, Finland:1699 –Undersökningen är genomförd under perioden 4 -10 januari 2010 YouGov källa.

58
Sexfrekvens

59
Seksfrekvens 15-20 år YouGov Kådiskollen 2010, RFSU

61
Oskyddad sex 15-20 år YouGov Kådiskollen 2010, RFSU

62
Osmo Kontula, Väestöliitto 2008 Accept parallell sexual relations among married people, women

63
Conclusions When adolescent sexuality is not condemned but sexuality education and sexual health services are provided, it is possible to profoundly improve adolescent sexual health with comparatively small costs. But each year new groups of young people mature, requiring new efforts. Education, counseling and services are all needed. If the resources are cut too much or not given, negative effects are soon evident. Political commitment and resources provided are reflected in results obtained Political commitment and resources provided are reflected in results obtained

64
Sammandrag, Finland Sedan 1970-talet satsning på användande av preventivmedel, inklusive kondom, som viktigt Hälsovårdspersonal skolad för detta Sedan 1960-talet nationell välfungerande papa screening Sedan 2004 bra sexualundervisning i skolorna Attityder mer konservativa? Mindre sex??

65
Sexual Health Clinic

Liknande presentationer