Ladda ner presentationen
Presentation laddar. Vänta.

1
João Fernandes ST-Läkare Neuro & Rehab Klinik – NÄL AT-dag Neurologi
Akut Neurologi João Fernandes ST-Läkare Neuro & Rehab Klinik – NÄL AT-dag Neurologi

2
Innehåll Konfusion Epilepsi vs Synkope Yrsel Stroke

3
“When you hear hoofbeats, think of horses not zebras”
Theodore Woodward

4
Konfusion Medvetandet Sensorium Vakenhet Klarhet Självmedvetande

5
Konfusion Medvetenhet Klarhet Vakenhet

6
Konfusion Vad kännetecknar konfusion?
Grundläggande fysiopatologisk mekanism? Diagnostiska kriterier?

7
Konfusion Orsaker Infektion Metaboliska faktorer Organsvikt
Endokrinopati Näringsbrist Intoxikation och Utsättning Läkemedel Vaskulära händelser CNS neoplasi och trauma Epileptiska anfall Hypertonisk encefalopati

8
Konfusion Kliniska Manifestationer (pre-morbid status?) Förloppet
Uppmärksamhet Orientering Vakenhetsgrad Varseblivning Tankeförmåga och innehåll Emotionell kontroll Språkförmåga Sömnmönster

9
Konfusion Kliniska tecken Pupiller och ögonbotten Ögonrörelser
Motorfunktion Allmänundersökning

10
Konfusion LAB Elektrolyter Glukos Urea Kreatinin Blodstatus + Diff
Levestatus Koagulation Toxikologiska prover EKG LP CT

11
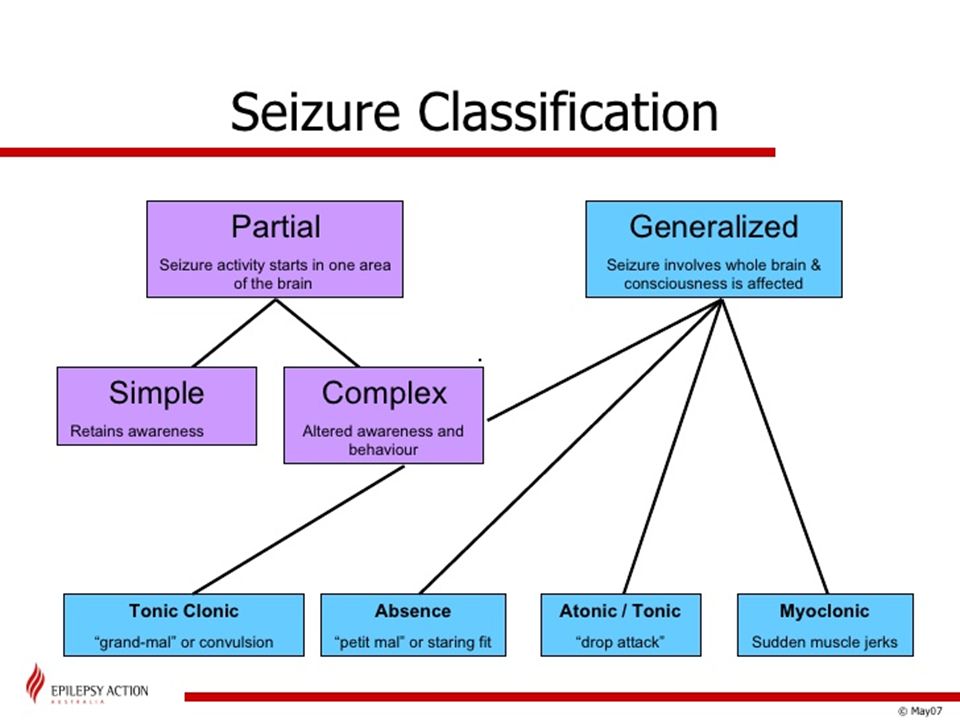
Krampanfall Grundläggande fysiopatologisk mekanism? Semiologi?
Varför är anfallens semiologi viktigt?

13
Krampanfall Etiologi Systemiska faktorer Läkemedel och toxiner
Utsättningssyndrom Infektion Vaskulär Trauma Neoplasi Idiopatisk Feber Genetiska syndrom

14
Synkope Definition Grundläggande fysiopatologisk mekanism?
Finns det utlösande faktorer?

15
Synkope Innan Synkope Efter

17
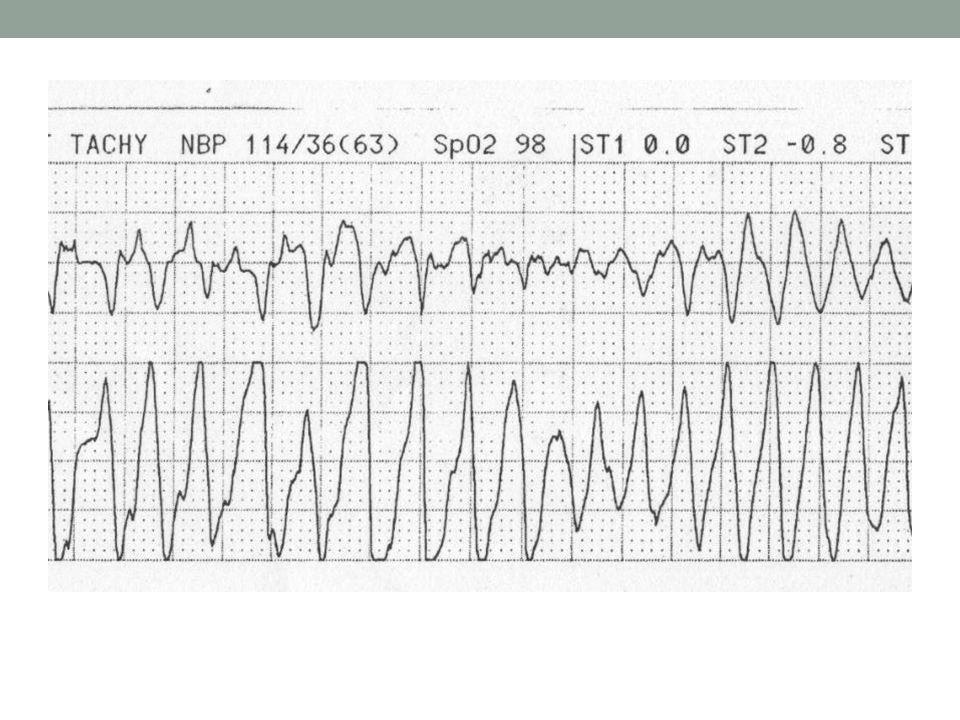
Synkope Orsaker Reflex medierad Ortostatisk Hyperventilation Kardiell
Neurocardiogenisk Situation betingad Carotid sinus syndrom Ortostatisk Hypoadrenergisk ortostatisk hypotension Postural tachycardia syndrom Hyperventilation Kardiell

18
Synkope Differentiell Diagnos Epilepsi Dropp attacks
Cataplexi (Narkolepsi) TIA?????
 TIA")
19
Yrsel Hur kan man skilja mellan central och perifer yrsel?
1) Vad menar patienterna när de klagar över yrsel? 2) Är yrsel fokusen i symptomatologin? 3) Klassifikation av den kliniska bilden a) svår långvarig yrsel b) Återkommande ställningsutlösta attacker c) Återkommande spontana yrselattacker 4) Nogrann neurologisk status 5) Neurootologisk undersökning
 Vad menar patienterna när de klagar över yrsel 2) Är yrsel fokusen i symptomatologin 3) Klassifikation av den kliniska bilden. a) svår långvarig yrsel. b) Återkommande ställningsutlösta attacker. c) Återkommande spontana yrselattacker. 4) Nogrann neurologisk status. 5) Neurootologisk undersökning.")
20
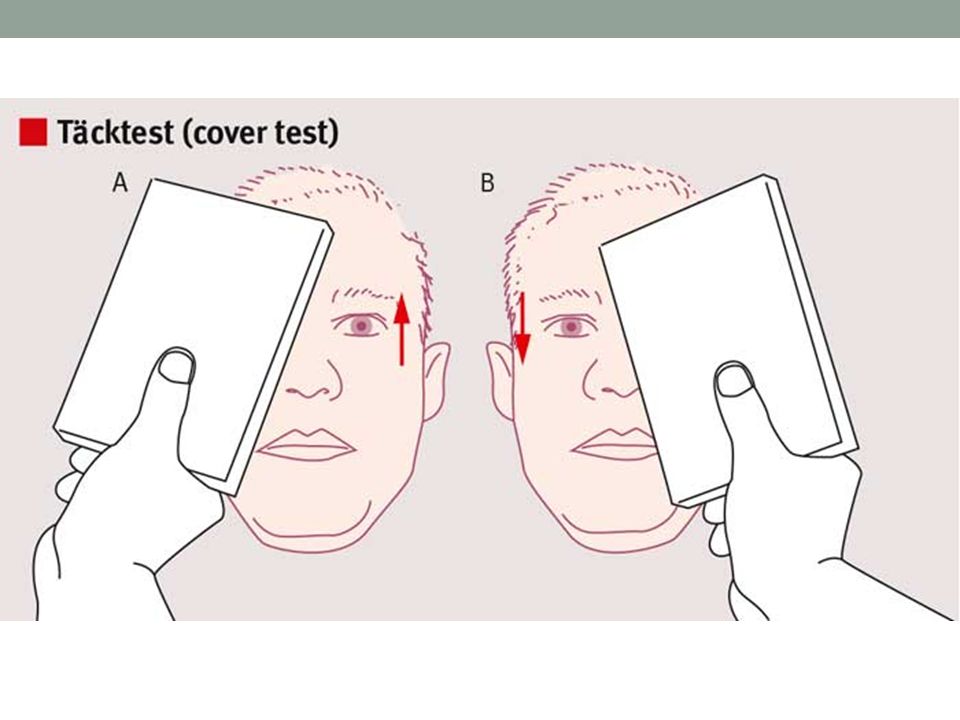
The head thrust test The head thrust test is a test of vestibular function that is performed as part of the bedside examination. The head thrust test The head thrust test is a test of vestibular function that is performed as part of the bedside examination. This maneuver tests the vestibulo-ocular reflex (VOR). The patient sits in front of the examiner and the examiner holds the patient's head steady in the midline. The patient is instructed to maintain gaze on the nose of the examiner. The examiner then quickly turns the patient's head about 10–15 degrees to one side and observes the ability of the patient to keep the eyes locked on the examiner's nose. Note that the test can also be performed by starting with the head turned to the side, and then making the quick movement back to the midline. If the patient's eyes stay locked on the examiner's nose (i.e., no corrective saccade) (A), then the peripheral vestibular system is assumed to be intact. Thus in a patient with acute dizziness, the absence of a corrective saccade suggests a CNS localization. If, however, the patient's eyes move with the head (B) and then the patient makes a voluntary eye movement back to the examiner's nose (i.e., corrective saccade), then this suggests a lesion of the peripheral vestibular system and not the CNS. When a patient presents with the acute vestibular syndrome, the test result shown in A would suggest a CNS lesion, whereas the test result in B would suggest a peripheral vestibular lesion (thus, vestibular neuritis). From: Edlow JA, Newman-Toker DE, Savitz SI. Diagnosis and initial management of cerebellar infarction. Lancet Neurol 2008;7:951–964. Kevin A. Kerber, and Robert W. Baloh Neurol Clin Pract 2011;1:24-33 Copyright © 2011 by AAN Enterprises, Inc.
. The patient sits in front of the examiner and the examiner holds the patient s head steady in the midline. The patient is instructed to maintain gaze on the nose of the examiner. The examiner then quickly turns the patient s head about 10–15 degrees to one side and observes the ability of the patient to keep the eyes locked on the examiner s nose. Note that the test can also be performed by starting with the head turned to the side, and then making the quick movement back to the midline. If the patient s eyes stay locked on the examiner s nose (i.e., no corrective saccade) (A), then the peripheral vestibular system is assumed to be intact. Thus in a patient with acute dizziness, the absence of a corrective saccade suggests a CNS localization. If, however, the patient s eyes move with the head (B) and then the patient makes a voluntary eye movement back to the examiner s nose (i.e., corrective saccade), then this suggests a lesion of the peripheral vestibular system and not the CNS. When a patient presents with the acute vestibular syndrome, the test result shown in A would suggest a CNS lesion, whereas the test result in B would suggest a peripheral vestibular lesion (thus, vestibular neuritis). From: Edlow JA, Newman-Toker DE, Savitz SI. Diagnosis and initial management of cerebellar infarction. Lancet Neurol 2008;7:951–964. Kevin A. Kerber, and Robert W. Baloh Neurol Clin Pract 2011;1: Copyright © 2011 by AAN Enterprises, Inc.")
24
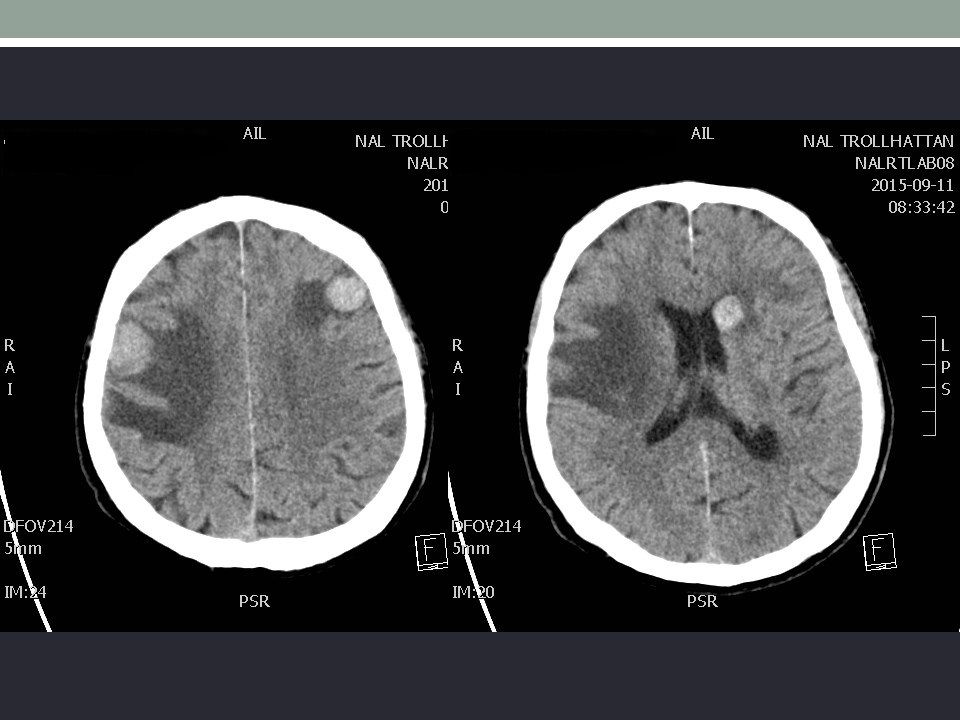
Stroke TIA är hjärnans “instabil angina”.
Finns det vaskulära riskfaktorer? Tidsförlopp Snabb utredning och diagnostik har stora konsekvenser. Varför bör man göra en CT?

26
Stroke Symtom och kärlområde (främre eller bakre cirkulation?)
Differentiell Diagnos Blodtryck?

Liknande presentationer




















 SSADM (1981) SSM (1966)RUP (1998) Ethics (1985) Agile (2001)>")