Ladda ner presentationen
Presentation laddar. Vänta.

1
Ge järnet En Odyssé i den anemiska skärgården med järnet som kompass
Pierre Blaud 1832 Michael Hedenus Med klin Sundsvall

2
Disclosures Konsultuppdrag/advisory board/betalda föreläsningar;
Vifor Pharma Pharmacosmos Takeda SBU

3
Cancer-relaterad anemi
ACD (Anemia of chronic disease) CIA (chemotherapy induced anemia) Andra orsaker har uteslutits såsom: Järnbrist (absolut) Hemolys B12/folat-brist
 CIA (chemotherapy induced anemia) Andra orsaker har uteslutits såsom: Järnbrist (absolut) Hemolys. B12/folat-brist.")
4
Patofysiologi av ACD Anemia of chronic disease
Agens Tumörcell Fas-L/TRAIL AIS Erytroblaster Erytrocyter Aktiverat immunsystem TNF- IFN- Makrofager TNF- IL-1 IFN- 1-anti- trypsin IL-6 Förkortad överlevnad Lever Neopterin TNF- IFN-, TNF- IL-1 IFN-, Hepcidin Minskad Hämmad Funktionell järnbrist erytropoetin- BFU-E produktion CFU-E Anemi Nowrousian MR et al. Marcel Dekker New York Basel 1996 and Springer Wien, New York 2007 4

5
Är cancer-relaterad anemi vanlig
Är cancer-relaterad anemi vanlig? European Cancer Anaemia treatment of anaemia survey Ludwig H, 2004 Anaemia prevalence in different cancer types Survey (ECAS) was a prospective epidemiology, observational survey conducted in 24 European countries to evaluate the prevalence, incidence anThe European Cancer Anaemia d treatment of anaemia (defined as haemoglobin <12.0g/dL) Data was obtained from 748 cancer centres with over 1,000 participating physicians Data collected included demographics, tumour type, performance status and haemoglobin (Hb) levels, cancer treatments and anaemia treatments Patients were evaluated for up to 6 months Anaemia was most frequent in patients with gynaecological cancer (81%) and lung cancer (77%); Of these patients Hb levels were between g/dL in 57% gynaecological patients and in 54% lung cancer patients (not shown in slide) Hb levels between g/dL were frequent in gynaecological patients (35%) and lung cancer patients (39%). The remaining lung and gynaecology patients had Hb levels <8.0g/dL (not shown in slide) Of the 15,367 patients enrolled: 14,912 were available for evaluation and 39.3% were anaemic. Most patients (29.3%) had mild anaemia (Hb between g/dL; moderate anaemia occurred in 8.7% (Hb g/dL) and severe anaemia in 1.3% (Hb< 8g/dL) This slide shows haemoglobin levels at enrollment according to tumour type. Data is based on an evaluable population of 14,912 of which there was missing/uncategorised data in 1,248 patients 1. Ludwig H, Van Belle S, Barrett-Lee P et al. Eur J Cancer 2004;40: 5
 was a prospective epidemiology, observational survey conducted in 24 European countries to evaluate the prevalence, incidence anThe European Cancer Anaemia d treatment of anaemia (defined as haemoglobin <12.0g/dL) Data was obtained from 748 cancer centres with over 1,000 participating physicians. Data collected included demographics, tumour type, performance status and haemoglobin (Hb) levels, cancer treatments and anaemia treatments. Patients were evaluated for up to 6 months. Anaemia was most frequent in patients with gynaecological cancer (81%) and lung cancer (77%); Of these patients Hb levels were between g/dL in 57% gynaecological patients and in 54% lung cancer patients (not shown in slide) Hb levels between g/dL were frequent in gynaecological patients (35%) and lung cancer patients (39%). The remaining lung and gynaecology patients had Hb levels <8.0g/dL (not shown in slide) Of the 15,367 patients enrolled: 14,912 were available for evaluation and 39.3% were anaemic. Most patients (29.3%) had mild anaemia (Hb between g/dL; moderate anaemia occurred in 8.7% (Hb g/dL) and severe anaemia in 1.3% (Hb< 8g/dL) This slide shows haemoglobin levels at enrollment according to tumour type. Data is based on an evaluable population of 14,912 of which there was missing/uncategorised data in 1,248 patients. 1. Ludwig H, Van Belle S, Barrett-Lee P et al. Eur J Cancer 2004;40:")
6
Är cancer-relaterad anemi ett problem?
Comparison of fatigue in the general population with fatigue in cancer patients1,2 FACT- Fatigue subscale Group General population n=1,010 Non-anaemic cancer patients n=113 Anaemic cancer patients n=2,292b F (post-hoc) Mean (SD)a 43.6 (9.4) 40.0 (9.8) 23.8 (12.6) 1,071.8b, G>N>A Median 47 42 23 - Range 2-52 9-52 0-52 FACT is the Functional Assessment of Cancer Therapy – the fatigue scales consist of 13 items The general population reported less fatigue ( they had higher values of the FACT-fatigue subscale than in either of the two cancer groups When gender, age and HB values were analysed using regression analysis to predict fatigue in cancer patients, Hb level was the only significant predictor of fatigue, accounting for 8% of the variance in fatigue score 1. Butt Z & Cella D. Chapter 14: Relationship of haemoglobin, fatigue, and quality of life in anaemic cancer patients, pp in Recombinant Human Erythropoietin (rhEPO) in Clinical Oncology. Scientific and clinical Aspects of Anemia in Cancer. Ed. M.R. Nowrousian,2nd edition 2008 2. Cella D, Peterman A, Passik S et al. Cancer 2002;94: Adapted by Butt Z & Cella D from Cella, Lai, Chang et al. 2002 a. Higher values indicated a better quality of life score/less fatigue; b Of the 2,369 anaemic patients, 97% completed a baseline questionnaires: b p<0.001 Hb level was the only significant predictor of fatigue in anaemic cancer patients 6
 Mean (SD)a (9.4) 40.0 (9.8) 23.8 (12.6) 1,071.8b, G>N>A. Median Range FACT is the Functional Assessment of Cancer Therapy – the fatigue scales consist of 13 items. The general population reported less fatigue ( they had higher values of the FACT-fatigue subscale than in either of the two cancer groups. When gender, age and HB values were analysed using regression analysis to predict fatigue in cancer patients, Hb level was the only significant predictor of fatigue, accounting for 8% of the variance in fatigue score. 1. Butt Z & Cella D. Chapter 14: Relationship of haemoglobin, fatigue, and quality of life in anaemic cancer patients, pp in Recombinant Human Erythropoietin (rhEPO) in Clinical Oncology. Scientific and clinical Aspects of Anemia in Cancer. Ed. M.R. Nowrousian,2nd edition Cella D, Peterman A, Passik S et al. Cancer 2002;94: Adapted by Butt Z & Cella D from Cella, Lai, Chang et al a. Higher values indicated a better quality of life score/less fatigue; b Of the 2,369 anaemic patients, 97% completed a baseline questionnaires: b p< Hb level was the only significant predictor of fatigue in anaemic cancer patients. 6.")
7
Fatigue better tolerated by doctors than by their patients
“What is more important to be reduced or relieved by treatment: fatigue, pain or both equally?” 20 40 60 80 100 Oncologists Patients Response (%) Fatigue Pain Both equally 41 34 6 5 94 1 Vogelzang N et al. Semin Hematol 1997;34 (suppl 2):4-12
 Fatigue. Pain. Both equally Vogelzang N et al. Semin Hematol 1997;34 (suppl 2):4-12.")
8
Onco-haematologists from nine European countries (n=375) were surveyed 2011 on their last five cancer patients treated for CIA (n=1730). Hedenus M et al; submitted for publication 2013

9
Blod transfusion Snabbaste sättet att höja Hb-nivån !! Men……
Övergående effekt Svårt att uppnå en långvarig stabil Hb-nivå Billigt? Ofarligt? Hedenus 2006

10
Anaemic oncology patients:3 hospitals in Sweden
S-vall

12
Årliga transfusioner cirka 30 miljoner enheter
Fatalities Reported to FDA Following Blood Transfusion Årliga transfusioner cirka 30 miljoner enheter Rapporterade dödsfall 177 TRALI = Transfusion Related Acute Lung Injury TACO = Transfusion Associated Circulatory Overload HTR = Hemolytic Transfusion Reactions

13
© Axel Hofmann – EHA Barcelona 2010
? HIV, HCV, HBV Emerging and infectious agents Prions (vCJD) Dengue (DENV) Babesia species Potential for severe clinical outcomes Chikungunya (CHIKV) St Louis encephalitis virus (SLEV) Leishmania species Trypanosoma cruzi Might support elevation to a higher priority in the future Prions (chronic wasting disease) Human herpesvirus 8 (HHV-8) HIV variants Human parovirus B19 Influenza A virus, subtype H5N1 Simian foamy virus (SFV) Borrelia burgdorferi Hepatitis A virus 1. Low to high 2. Sufficient 3. Absent to low Carries public and/or regulatory concern Stramer, SL et al. Emerging infectious disease agents and their potential threat to transfusion safety. Transfusion, Suppl 2: p © Axel Hofmann – EHA Barcelona 2010 13
 Dengue (DENV) Babesia species. Potential for severe. clinical outcomes. Chikungunya (CHIKV) St Louis encephalitis virus (SLEV) Leishmania species. Trypanosoma cruzi. Might support elevation to a higher. priority in the future. Prions (chronic wasting disease) Human herpesvirus 8 (HHV-8) HIV variants. Human parovirus B19. Influenza A virus, subtype H5N1. Simian foamy virus (SFV) Borrelia burgdorferi. Hepatitis A virus. 1. Low to high. 2. Sufficient. 3. Absent to low. Carries public and/or. regulatory concern. Stramer, SL et al. Emerging infectious disease agents and. their potential threat to transfusion safety. Transfusion, Suppl 2: p © Axel Hofmann – EHA Barcelona")
14
subject to modification as circumstances change
Borna disease virus (t) Classical CJD Colorado tick fever virus (vl) Crimean-Congo hemorrhagic fever virus (t) Eastern equine encephalitis virus (t) Ebola virus (t) Enteroviruses (t) Epstein-Barr virus (vl) GB/HG viruses (a) Hantavirus New World (t) Hantavirus Old World (t) HBV variants (vl) HEV (vl) Herpes viruses (other than CMV, EBV, HHV-8) (t) HTLV variants (t) Influenza A and B viruses (other than H5N1 (t) Japanese encephalitis virus (t) La Crosse virus (t) Lassa virus (t) Lymphocytic choriomeningitis virus Marburg virus (t) Monkeypox virus (t) Mumps virus (t) Papillomaviruses (t) Polyomaviruses (t) Porcine endogenous retrovirus (t) Porcine parovirus (t) Rhabdovirus (a) SARS coronavirus (t) Tick-borne encephalitis virus complex (vl) Torque teno (TTV/TTLV/SEN-V) Vaccinia virus (t) Variola virus (t) Western equine encephalitis virus (t) XMRV? and what is next ? Courtesy © Axel Hofmann – EHA Barcelona 2010 Watch list subject to modification as circumstances change Stramer, SL et al. Emerging infectious disease agents and their potential threat to transfusion safety. Transfusion, Suppl 2: p 14
 Classical CJD. Colorado tick fever virus (vl) Crimean-Congo hemorrhagic fever virus (t) Eastern equine encephalitis virus (t) Ebola virus (t) Enteroviruses (t) Epstein-Barr virus (vl) GB/HG viruses (a) Hantavirus New World (t) Hantavirus Old World (t) HBV variants (vl) HEV (vl) Herpes viruses (other than CMV, EBV, HHV-8) (t) HTLV variants (t) Influenza A and B viruses (other than H5N1 (t) Japanese encephalitis virus (t) La Crosse virus (t) Lassa virus (t) Lymphocytic choriomeningitis virus. Marburg virus (t) Monkeypox virus (t) Mumps virus (t) Papillomaviruses (t) Polyomaviruses (t) Porcine endogenous retrovirus (t) Porcine parovirus (t) Rhabdovirus (a) SARS coronavirus (t) Tick-borne encephalitis virus complex (vl) Torque teno (TTV/TTLV/SEN-V) Vaccinia virus (t) Variola virus (t) Western equine encephalitis virus (t) XMRV and what is next Courtesy © Axel Hofmann – EHA Barcelona Watch list. subject to modification as circumstances change. Stramer, SL et al. Emerging infectious disease agents. and their potential threat to transfusion safety. Transfusion, Suppl 2: p")
15
Cox multiregressionsanalys- blodtransf. oberoende faktor
Blodtransfusion anemiska cancerpatienter Khorana A et al Arch Intern Med/vol 168 ( 21), nov 24, 2008 Retrospektiv kohortstudie N ( USA) VTE: RBC tx 7,2 % vs kontroll 3,8% OR VTE 1,60 (95% CI 1,53-1,67) OR Mortalitet 1,34 (95% CI 1,29-1,38) Cox multiregressionsanalys- blodtransf. oberoende faktor 15
, nov 24, Retrospektiv kohortstudie. N ( USA) VTE: RBC tx 7,2 % vs kontroll 3,8% OR VTE 1,60 (95% CI 1,53-1,67) OR Mortalitet 1,34 (95% CI 1,29-1,38) Cox multiregressionsanalys- blodtransf. oberoende faktor. 15.")
16
Patofysiologi av ACD Anemia of chronic disease
Agens Tumörcell Fas-L/TRAIL AIS Erytroblaster Erytrocyter Aktiverat immunsystem TNF- IFN- Makrofager TNF- IL-1 IFN- 1-anti- trypsin IL-6 Förkortad överlevnad Lever Neopterin TNF- IFN-, TNF- IL-1 IFN-, Hepcidin Minskad Hämmad Funktionell järnbrist erytropoetin- BFU-E produktion CFU-E Anemi Nowrousian MR et al. Marcel Dekker New York Basel 1996 and Springer Wien, New York 2007 16

17
A 4 Darbepoetin alfa Placebo 3 2 1 Change in Hb (g/dL) –1 –2
Change in Hb over time in CIA LPD patients Hedenus et al Br J Haematol 2003;122: 4 3 2 1 –1 –2 Darbepoetin alfa Placebo Change in Hb (g/dL) A -[Taken from 161 Core Slide Kit] Key point Median change in haemoglobin (Hb) over time curves started to separate as early as week 3. The darbepoetin alfa curve remained consistently higher than the placebo curve until end of treatment phase. Background The median change in Hb over time was calculated by subtracting each patient’s baseline Hb value from their Hb value at each time point, and taking a median of all patients. Hb values within 28 days of a red blood cell (RBC) transfusion were excluded. No missing values were imputed for this analysis, thus the population size fluctuated between time points, and gradually decreased as patients withdrew from the study. Treatment duration (weeks) Placebo n = Darbepoetin alfa n = 95% confidence interval for the median .
 A -[Taken from 161 Core Slide Kit] Key point. Median change in haemoglobin (Hb) over time curves started to separate as early as week 3. The darbepoetin alfa curve remained consistently higher than the placebo curve until end of treatment phase. Background. The median change in Hb over time was calculated by subtracting each patient’s baseline Hb value from their Hb value at each time point, and taking a median of all patients. Hb values within 28 days of a red blood cell (RBC) transfusion were excluded. No missing values were imputed for this analysis, thus the population size fluctuated between time points, and gradually decreased as patients withdrew from the study Treatment duration (weeks) Placebo n = Darbepoetin alfa n = % confidence interval for the median. .")
18
Mean (95% Cl) change in FACT-F subscale score
Fatigue can be reversed with ESA:s Mean change in FACT-F subscale score Hedenus M, et al. Hematol J. 2003;4(suppl 2):255.. 5 P = 0.032 n = 152 4 Mean (95% Cl) change in FACT-F subscale score 3 2.88 n = 151 2 A - Taken from 161 Core Slide Kit Key point After adjusting for the effect of baseline score, treatment with darbepoetin alfa significantly increased Functional Assessment of Cancer Therapy-Fatigue (FACT-F) subscale scores when compared with placebo (P = 0.032). Background 84% of patients completed the FACT-F scale at week 13, representing a high degree of compliance. Patients with the highest levels of fatigue at baseline (ie, lowest baseline FACT-F scale scores) reported the greatest improvement in scores at the end of treatment. A significant relationship was observed between change in haemoglobin (Hb) and change in FACT-F during the treatment period (P <0.001). For every 1 g/dL increase in Hb, the estimated mean increase in FACT-F scale score was 1.39 (95% confidence interval [CI]: 0.83, 1.94). 1 0.60 Darbepoetin alfa Placebo 18
: P = n = Mean (95% Cl) change in FACT-F subscale score n = A - Taken from 161 Core Slide Kit. Key point. After adjusting for the effect of baseline score, treatment with darbepoetin alfa significantly increased Functional Assessment of Cancer Therapy-Fatigue (FACT-F) subscale scores when compared with placebo (P = 0.032). Background. 84% of patients completed the FACT-F scale at week 13, representing a high degree of compliance. Patients with the highest levels of fatigue at baseline (ie, lowest baseline FACT-F scale scores) reported the greatest improvement in scores at the end of treatment. A significant relationship was observed between change in haemoglobin (Hb) and change in FACT-F during the treatment period (P <0.001). For every 1 g/dL increase in Hb, the estimated mean increase in FACT-F scale score was 1.39 (95% confidence interval [CI]: 0.83, 1.94) Darbepoetin alfa. Placebo. 18.")
19
RBC transfusions LPD studies
Hedenus M et al; Leuk Lymphoma Nov;53(11):
:")
20
Overall Survival in Patients with CIA Lymphoid Malignancies (FU 2 years)
100 Darbepoetin alfa Placebo 80 60 Percent 40 Total Deaths Hazard Ratio1 Darbepoetin Placebo 20 1.33 (95% CI: 0.95, 1.86) On this slide, we observe no convincing evidence for significant decrease in overall survival in association with Aranesp® (darbepoetin alfa) therapy. Again the hazard ratio is above one, but the confidence interval extends below one. I will now review the pooled analysis for these completed trials. 3 6 9 12 15 18 21 24 Months from 1st Dose Subjects at risk: Darbepoetin 175 162 150 136 126 122 117 101 76 Placebo 169 160 146 135 132 124 116 113 93 1Adjusted for disease type, stage and IPI score Hedenus M et al. J Clin Oncol 2005;23:6941–6948
 On this slide, we observe no convincing evidence for significant decrease in overall survival in association with Aranesp® (darbepoetin alfa) therapy. Again the hazard ratio is above one, but the confidence interval extends below one. I will now review the pooled analysis for these completed trials Months from 1st Dose. Subjects at risk: Darbepoetin Placebo Adjusted for disease type, stage and IPI score. Hedenus M et al. J Clin Oncol 2005;23:6941–6948.")
21
Hedenus M et al. J Clin Oncol 2005;23:6941–6948
Prolongation of longterm FU (3 years) HR 1.36(95% CI: ) ODAC meeting 2006
 HR 1.36(95% CI: ) ODAC meeting")
22
Metaanalys OS LPD OR 1,04 (95%CI: 0,81-1. 34) 95% CI: 0. 95, 1. 86) 1
Metaanalys OS LPD OR 1,04 (95%CI: 0, ) 95% CI: 0.95, 1.86) 1.33 (95% CI: 0.95, 1.86) 1.33 (95% CI: 0.95, 1.86) Hedenus M et al; Leuk Lymphoma Nov;53(11):
 95% CI: 0.95, 1.86) 1.33 (95% CI: 0.95, 1.86) 1.33 (95% CI: 0.95, 1.86) Hedenus M et al; Leuk Lymphoma Nov;53(11):")
23
Cochrane meta-analysis 2006: VTE - RR 1.67
Study Treatment Control n/N n/N Thatcher 1999a (37) 0/42 0/22 Cascinu 1994 (12) 0/50 0/50 EPO-CAN-20 J&J (62) 1/31 2/31 Case J&J (13) 2/81 3/76 Henry J&J (14) 6/67 8/65 N FDA (66) 24/109 26/115 Chang 2005 (48) 19/175 14/175 Littlewood J&J (6) 14/251 5/124 Vansteenkiste 2002 (53) 7/155 5/159 INT-1 J&J (64) 3/164 1/80 Witzig J&J (46) 9/168 6/165 Osterborg 1996b (24) 1/48 0/24 Ten Bokkel 1998a (31) 2/45 0/17 Thatcher 1999b (37) 2/44 0/22 Osterborg 1996a (24) 2/47 0/25 Abels J&J (15) 1/65 0/59 Welch 1995 (38) 1/15 0/15 Ten Bokkel 1998b (31) 4/42 0/16 INT-3 J&J (65) 8/135 1/65 Savonije 2004 (51) 9/211 1/104 Dammacco J&J (20) 5/69 1/76 P-174 J&J (16) 0/33 0/12 Bamias 2003 (47) 0/72 1/72 Smith 2003 (45) 1/64 1/22 Thompson 2000 (27) 1/45 0/21 Leyland-Jones J&J (8) 36/448 25/456 Henke 2003 Roche (7) 10/180 6/171 Rose J&J (17) 9/142 2/79 Throuvalas 2000 (32) 1/28 0/26 GOG-0191 FDA (63) 9/58 3/55 Italian 1998 (21) 1/44 0/43 Razzouk 2004 (44) 6/112 2/110 Osterborg 2002 (25) 1/170 0/173 Vadhan-Raj FDA (56) 7/29 2/31 Machtay 2004 (54) 2/71 0/70 EPO-GBR-7 FDA (57) 5/151 1/149 EPO-CAN-15 FDA (61) 16/53 2/53 Rosenzweig 2004 (60) 4/14 0/13 Total (95% CI) Total events: 229 (treatment), 118 (control) Weight RR (fixed) % 95% CI Not estimable (0.05, 5.23) (0.11, 3.64) (0.27, 1.98) (0.60, 1.59) (0.70, 2.62) (0.51, 3.75) (0.47, 4.43) (0.15, 13.85) (0.54, 4.05) (0.06, 36.23) (0.10, 38.79) (0.13, 51.05) (0.14, 54.32) (0.11, 65.68) (0.13, 68.26) (0.20, 62.58) (0.49, 30.15) (0.57, 34.55) (0.66, 45.98) (0.01, 8.05) (0.02, 5.27) (0.06, 33.82) (0.89, 2.40) (0.59, 4.26) (0.55, 11.30) (0.12, 65.66) (0.81, 9.96) (0.12, 70.08) (0.61, 14.28) (0.13, 74.41) (0.85, 16.56) (0.24, ) (0.58, 41.73) (1.93, 33.09) (0.50, ) (1.35, 2.06) 0.01 0.1 10 ESA Treatment Control 100 1/3 off label Please see excel spreadsheet for details on studies. The meta-analysis on Epoetin alfa only studies showed the same risk for TVEs (1.42 or 1.48) as did the Cochrane meta-analysis (1.47) across all ESA studies, within and outside labeling. VTE, venous thromboembolic events; RR, relative risk Bohlius J et al. J Natl Cancer Inst 2006;98:708–714 23
 0/42 0/22. Cascinu 1994 (12) 0/50 0/50. EPO-CAN-20 J&J (62) 1/31 2/31. Case J&J (13) 2/81 3/76. Henry J&J (14) 6/67 8/65. N FDA (66) 24/109 26/115. Chang 2005 (48) 19/175 14/175. Littlewood J&J (6) 14/251 5/124. Vansteenkiste 2002 (53) 7/155 5/159. INT-1 J&J (64) 3/164 1/80. Witzig J&J (46) 9/168 6/165. Osterborg 1996b (24) 1/48 0/24. Ten Bokkel 1998a (31) 2/45 0/17. Thatcher 1999b (37) 2/44 0/22. Osterborg 1996a (24) 2/47 0/25. Abels J&J (15) 1/65 0/59. Welch 1995 (38) 1/15 0/15. Ten Bokkel 1998b (31) 4/42 0/16. INT-3 J&J (65) 8/135 1/65. Savonije 2004 (51) 9/211 1/104. Dammacco J&J (20) 5/69 1/76. P-174 J&J (16) 0/33 0/12. Bamias 2003 (47) 0/72 1/72. Smith 2003 (45) 1/64 1/22. Thompson 2000 (27) 1/45 0/21. Leyland-Jones J&J (8) 36/448 25/456. Henke 2003 Roche (7) 10/180 6/171. Rose J&J (17) 9/142 2/79. Throuvalas 2000 (32) 1/28 0/26. GOG-0191 FDA (63) 9/58 3/55. Italian 1998 (21) 1/44 0/43. Razzouk 2004 (44) 6/112 2/110. Osterborg 2002 (25) 1/170 0/173. Vadhan-Raj FDA (56) 7/29 2/31. Machtay 2004 (54) 2/71 0/70. EPO-GBR-7 FDA (57) 5/151 1/149. EPO-CAN-15 FDA (61) 16/53 2/53. Rosenzweig 2004 (60) 4/14 0/13. Total (95% CI) Total events: 229 (treatment), 118 (control) Weight RR (fixed) % 95% CI. Not estimable (0.05, 5.23) (0.11, 3.64) (0.27, 1.98) (0.60, 1.59) (0.70, 2.62) (0.51, 3.75) (0.47, 4.43) (0.15, 13.85) (0.54, 4.05) (0.06, 36.23) (0.10, 38.79) (0.13, 51.05) (0.14, 54.32) (0.11, 65.68) (0.13, 68.26) (0.20, 62.58) (0.49, 30.15) (0.57, 34.55) (0.66, 45.98) (0.01, 8.05) (0.02, 5.27) (0.06, 33.82) (0.89, 2.40) (0.59, 4.26) (0.55, 11.30) (0.12, 65.66) (0.81, 9.96) (0.12, 70.08) (0.61, 14.28) (0.13, 74.41) (0.85, 16.56) (0.24, ) (0.58, 41.73) (1.93, 33.09) (0.50, ) (1.35, 2.06) ESA Treatment. Control /3 off label. Please see excel spreadsheet for details on studies. The meta-analysis on Epoetin alfa only studies showed the same risk for TVEs (1.42 or 1.48) as did the Cochrane meta-analysis (1.47) across all ESA studies, within and outside labeling. VTE, venous thromboembolic events; RR, relative risk. Bohlius J et al. J Natl Cancer Inst 2006;98:708–")
24
Men endast 50-65% svarar på EPO.
Hedenus M et al. J Clin Oncol 2005;23:6941–6948 Darbepoetin alfa Placebo P <0.001 P <0.001 P <0.001 n = 174 n = 86 n = 88 64 60 56 n = 86 Key points Darbepoetin alfa increased the percentage of patients achieving a Hb response to 60%, from 18% in the placebo group (P <0.001).1 When analysed by malignancy type, the difference between response rates in the darbepoetin alfa and placebo groups was significant in each case: lymphoma: darbepoetin alfa 64% vs placebo 13% (P <0.001) myeloma: darbepoetin alfa 56% vs placebo 23% (P <0.001).1 Background Previously published studies have suggested a possible difference in the Hb response rate between patients with multiple myeloma and lymphoma, although more recent studies have not supported this observation.2,3 In the present study, similar rates of response were seen in both sets of patients. References 1. Hedenus M, et al. Br J Haematol. In press. 2. Dammacco F, et al. Br J Haematol. 2001;113: 3. Österborg A, et al. J Clin Oncol. 2002;20: n = 170 n = 84 23 18 13 Overall Lymphoma Myeloma * Hemoglobin response is defined as an increase of 2 g/dL from baseline in the absence of any RBC transfusion within the preceding 28 days
.1. When analysed by malignancy type, the difference between response rates in the darbepoetin alfa and placebo groups was significant in each case: lymphoma: darbepoetin alfa 64% vs placebo 13% (P <0.001) myeloma: darbepoetin alfa 56% vs placebo 23% (P <0.001).1. Background. Previously published studies have suggested a possible difference in the Hb response rate between patients with multiple myeloma and lymphoma, although more recent studies have not supported this observation.2,3 In the present study, similar rates of response were seen in both sets of patients. References. 1. Hedenus M, et al. Br J Haematol. In press. 2. Dammacco F, et al. Br J Haematol. 2001;113: Österborg A, et al. J Clin Oncol. 2002;20: n = 170. n = Overall. Lymphoma. Myeloma. * Hemoglobin response is defined as an increase of 2 g/dL from baseline in the absence of any RBC transfusion within the preceding 28 days.")
25
Patofysiologi av ACD Anemia of chronic disease
Agens Tumörcell Fas-L/TRAIL AIS Erytroblaster Erytrocyter Aktiverat immunsystem TNF- IFN- Makrofager TNF- IL-1 IFN- 1-anti- trypsin IL-6 Förkortad överlevnad Lever Neopterin TNF- IFN-, TNF- IL-1 IFN-, Hepcidin Minskad Hämmad Funktionell järnbrist erytropoetin- BFU-E produktion CFU-E Anemi Nowrousian MR et al. Marcel Dekker New York Basel 1996 and Springer Wien, New York 2007 25 25

26
Iron-restricted erythropoises IRE
Absolut ID Funktionell ID Vid ACD EPO-behandling

27
Diagnosing absolute and functional iron deficiency
Absolute iron deficiency2 Functional iron deficiency 2,3 Normal1 Storage iron Transport iron Erythron iron Functional iron deficiency occurs when transferrin saturation levels are equal or fall below 20%. This indicates where there is sufficient iron available for production of RBCs Serum ferritin is a measure of the amount of available iron in storage sites such as the liver, kidney and spleen. In FID deficiency, iron stores are normal, but are not mobilised faster enough to meet the requirements for RBC production Renate H , Schaefer R. 2006 NCCN Guidelines 2008, 3. NCCN Guidelines V3, (men) (women) Serum Ferritin (ng/mL) <30 ≥1002 < 3003 Transferrin saturation (%) 20-45 ≤15 ≤20 Haemoglobin (g/dL) ≥12-13 <12-13 <12-13 1. Renate H, 2006; 2. NCCN Guidelines 2008; 3. NCCN Guideline 2009
 (women) Serum Ferritin (ng/mL) <30. ≥1002 < Transferrin saturation (%) ≤15. ≤20. Haemoglobin (g/dL) ≥ < < Renate H, 2006; 2. NCCN Guidelines 2008; 3. NCCN Guideline")
28
Mikrocytos, hypokromasi
Tar veckor att utveckla I allmänhet har patienten adapterat till sin låga Hb-nivå TSAT och ferritin Akuta fasreaktanter Beakta CRP!

29
Iron homeostasis in the healthy state
Stein et al. Nat Rev Gastroenterol Hepatol 2010

30
Erytropoes Fe, Folat, B12 Hematopoes Pluripotent stamcell Erytropoetin
transferrinreceptorer Erytropoetin BFU-E CFU-E T-cell B-cell Trombocyter Här ser vi stamcellsträdet. Dvs det är från den Pluripotenta stamcellen som alla celler bildas från. Det kroppsegna erytropoietinet, har sin verkan på denna röda cellinje i stamcellsträdet. BFU-E (erytroid burst forming units) och E-CFU (erytroid colony forming units) är förstadier till färdigutvecklade erytrocyter. På ytorna på de erytroida stamcellerna finns speciella receptorer. På dessa receptorer” sätter sig” EPO:t och det medför att dessa omogna erytrocyter vidareutveclas och utmognar så småningom till en färdig erytrocyt. Erytropoietinet ärhelt enkelt en överlevnadsfaktor för dessa omogna erytrocyter som skyddar cellmembranet. Annars dör en stor del av dessa celler på sin väg till mognad. Hur signalen överförs in till cellen är ännu okänt. (EPO verkar på tre nivåer: 1. Stimulerar cellbildningen 2. Stimulerar utmogningen av röda blodkroppar 3. Motverkar celldöd (apoptos) Viktigast! Dvs cellcykeln förlängs. Själva mognadsprocessen tar tid. Ca 14 dagar för reticulocyterna att nå blodbanan, (omogna röda blodkroppar) och när de förlorar sin cellkärna utmognar de till erytrocyter. Sedan tar det ytterligare 1-2 veckor för att man ska kunna mäta effekten i Hb. Erytropoietinet verkar enbart på den röda celllinjen – dvs därför får man ingen påverkan på övriga celler såsom trombocyter, neutrofila etc. Retikulocyter Basofila Neutrofila Erytrocyter Eosinofila Makrofager BFU-E = burst-forming unit–erythroid CFU-E = colony-forming unit–erythroid
 och E-CFU (erytroid colony forming units) är förstadier till färdigutvecklade erytrocyter. På ytorna på de erytroida stamcellerna finns speciella receptorer. På dessa receptorer sätter sig EPO:t och det medför att dessa omogna erytrocyter vidareutveclas och utmognar så småningom till en färdig erytrocyt. Erytropoietinet ärhelt enkelt en överlevnadsfaktor för dessa omogna erytrocyter som skyddar. cellmembranet. Annars dör en stor del av dessa celler på sin väg till mognad. Hur signalen överförs in till cellen är ännu okänt. (EPO verkar på tre nivåer: 1. Stimulerar cellbildningen. 2. Stimulerar utmogningen av röda blodkroppar. 3. Motverkar celldöd (apoptos) Viktigast! Dvs cellcykeln förlängs. Själva mognadsprocessen tar tid. Ca 14 dagar för reticulocyterna att nå blodbanan, (omogna röda blodkroppar) och när de förlorar sin cellkärna utmognar de till erytrocyter. Sedan tar det ytterligare 1-2 veckor för att man ska kunna mäta effekten i Hb. Erytropoietinet verkar enbart på den röda celllinjen – dvs därför får man ingen påverkan på övriga celler såsom trombocyter, neutrofila etc. Retikulocyter. Basofila. Neutrofila. Erytrocyter. Eosinofila. Makrofager. BFU-E = burst-forming unit–erythroid. CFU-E = colony-forming unit–erythroid.")
31
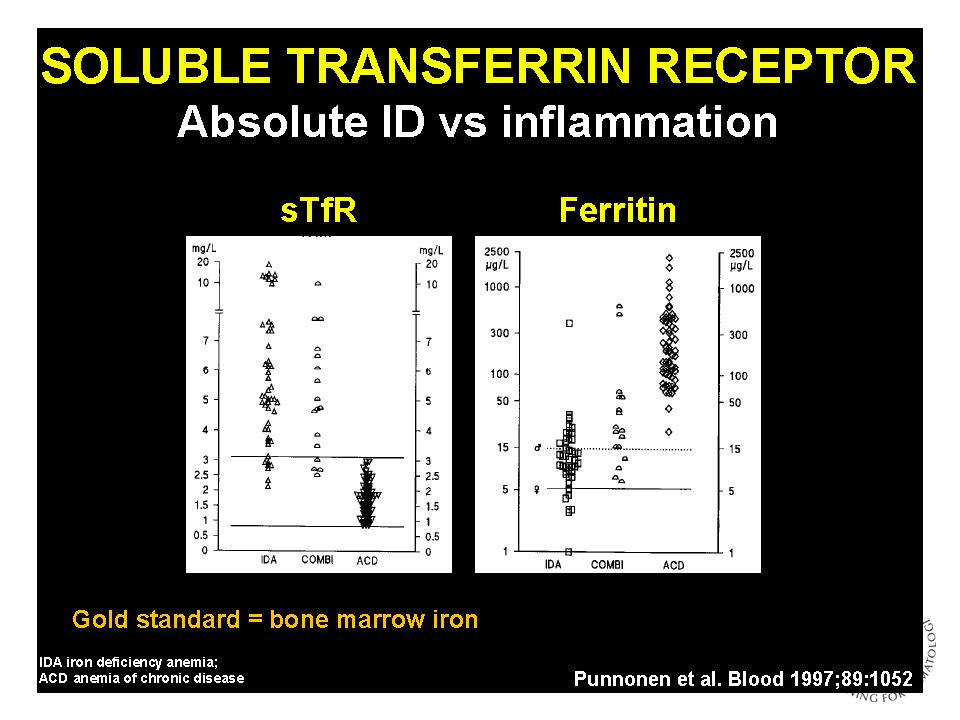
S-löslig transferrinreceptor
S-TfR TfR

33
Järndepå Ferritin Hemosiderin (”kroppens rost”)
Proteinskal omger en central kärna av järnhydroxidfosfat Järn frigörs vid behov Akut fasreaktant Hemosiderin (”kroppens rost”) Nedbrytningsprodukt av ferritin Heterogent konglomerat av järn och nedbrytningsprodukter från protein och cellmembran Svårmobiliserbart I cytosol
 Nedbrytningsprodukt av ferritin. Heterogent konglomerat av järn och nedbrytningsprodukter från protein och cellmembran. Svårmobiliserbart. I cytosol.")
34
Ferritin Är det rimligt med olika referensintervall för män och kvinnor ?
Beutler E. ASH slide-bank

35
Järntransport – Transferrin Transferrinbundet järn – 3-4 mg
Två binding-sites för Fe3+ Förebygger oxidativ stress Normalt är 30-40% av transferrinet mättat med Fe3+ Transferrinmättnad < 20% tyder på Järnbrist absolut/funktionell

36
Järnupptag huvudsakligen i duodenum
Järn i födoämnen Hemjärn (10%) Kött, blod, inälvsmat, fågel, fisk Upptag(15-35%) Ingen påverkan av kostfaktorer Ikke-hemjärn, jonisert trevärt järnhydroxid(90%) I både vegetabiliska och animala födoämnen Joniseras av magsyran Upptag påverkas av kost och läkemedel Svaga syror ökar upptaget Hemjern – ca 40% av jernet i disse matvarene er hemjern Ikke-hemjern – Medisiner som hemmer absorbsjon: PPI, antacida, tetracycliner Kostfaktorer som hemmer absorbsjon: calsium, polyfenoler (garvesyre i te og kaffe), fytinsyre i konprodukter Fremmer absorbsjon: Askorbinsyre, ”kjøttfaktor” (trolig et peptid)
 Kött, blod, inälvsmat, fågel, fisk. Upptag(15-35%) Ingen påverkan av kostfaktorer. Ikke-hemjärn, jonisert trevärt järnhydroxid(90%) I både vegetabiliska och animala födoämnen. Joniseras av magsyran. Upptag påverkas av kost och läkemedel. Svaga syror ökar upptaget. Hemjern – ca 40% av jernet i disse matvarene er hemjern. Ikke-hemjern – Medisiner som hemmer absorbsjon: PPI, antacida, tetracycliner. Kostfaktorer som hemmer absorbsjon: calsium, polyfenoler (garvesyre i te og kaffe), fytinsyre i konprodukter. Fremmer absorbsjon: Askorbinsyre, kjøttfaktor (trolig et peptid)")
37
Hämmar joniserat järnupptag från tarm
Protonpump-hämmare Antacida Tetracycliner Kalcium Fytinsyra - spannmål/kål Polyfenoler – te och kaffe Helicobacter pylori

38
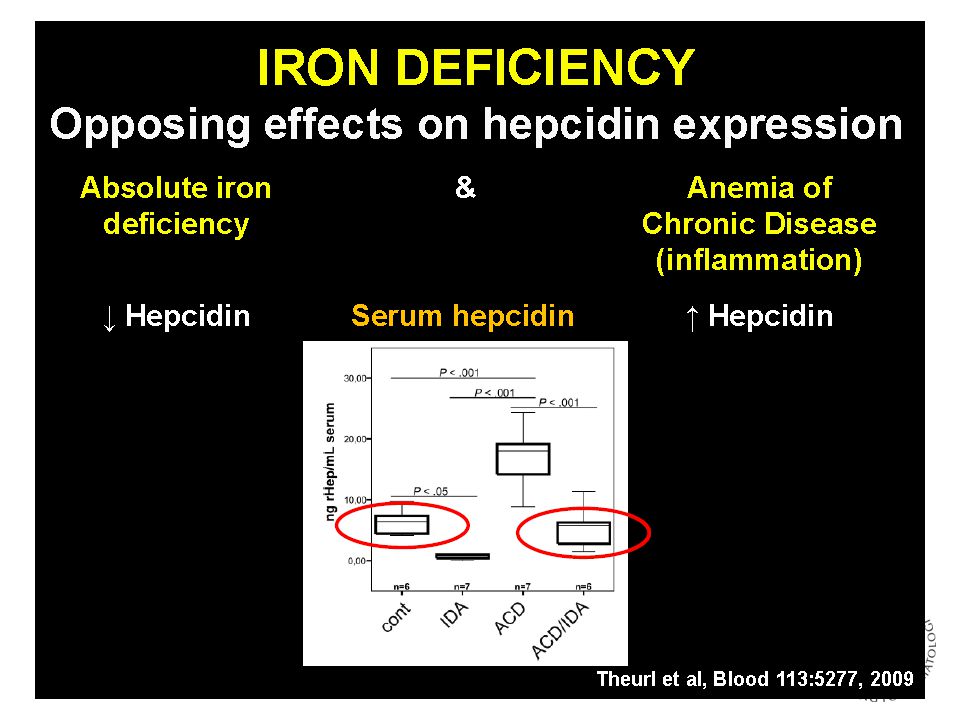
…och järnmetabolismens hjärna finns i levern
Makrofag S-Fe Lever Ferroportin Frisättning av järn Hepcidin Ferroportin Upptag av järn i tarmen Omarbetat efter Nemeth et al. J Clin Invest 2004;113:1271-6

39
Ganz. J Am Soc Nephrol 2007

41
Epo-behandling Normal Fe 30 mg/d Fe 60 mg/d Från Birgegård G
Erytropoes och järnbehov fördubblad Normal Fe 30 mg/d Fe 60 mg/d Från Birgegård G

42
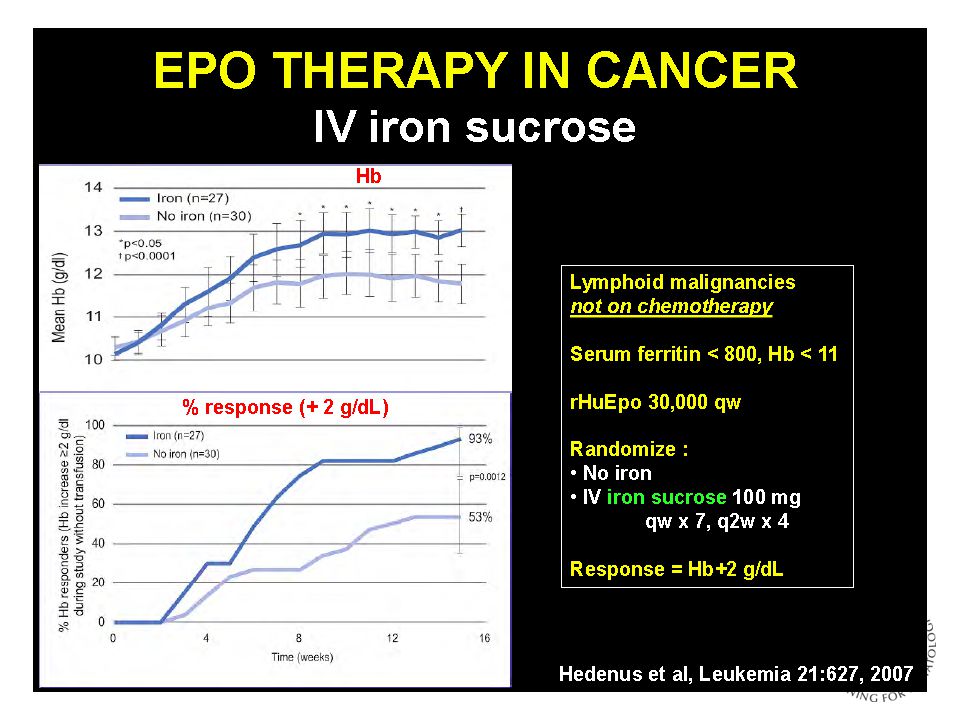
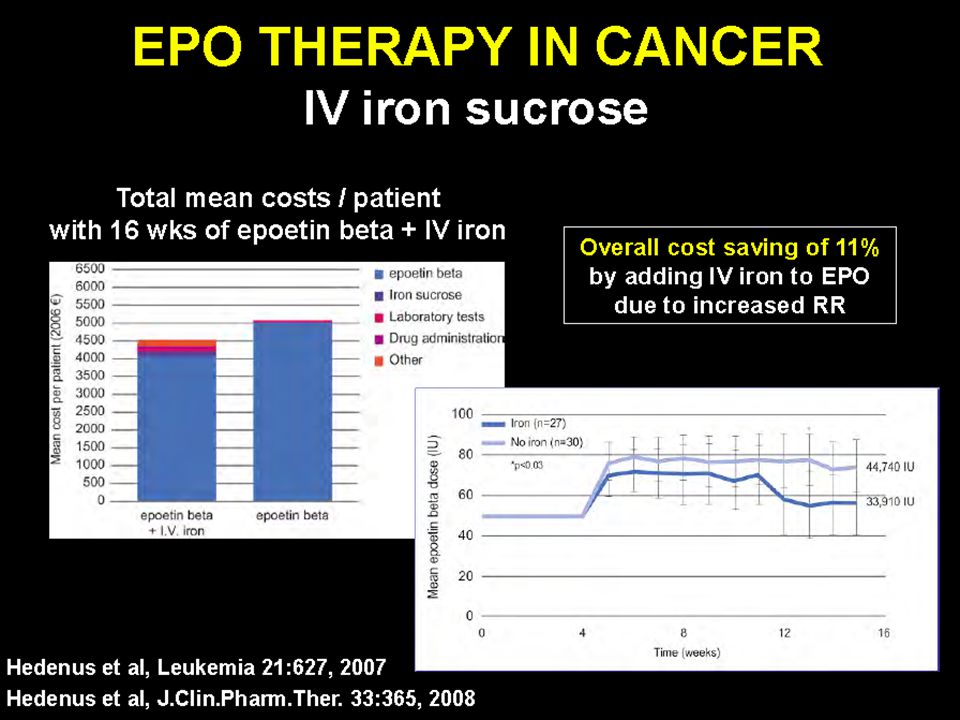
Effekt av EPO-beh +/- IV järn
Hedenus M et al; Leukemia Apr;21(4):627-32 Serum-ferritin TSAT TfR A third of patients in the non-iron group developed depleted iron stores (serum ferritin < 100μg/l) and only half of these patients had an increase in Hb >2g/dL during the study period In contrast, serum ferritin levels almost doubled during the study period and all patients with signs of FID at baseline responded with an increase in Hb >2g/dL in the IV iron group TSAT levels reflect iron availability TSAT levels were below 20% during the treatment period in 27/30 patients (86%) in the non-iron group in comparison with only 3/27 patients (11%) in the IV group These results indicate that the superior Hb response in the intravenous iron group was due to better availability of iron Reticulocytes Hedenus M et al. Leukemia 2007 42
: Serum-ferritin. TSAT. TfR. A third of patients in the non-iron group developed depleted iron stores (serum ferritin < 100μg/l) and only half of these patients had an increase in Hb >2g/dL during the study period. In contrast, serum ferritin levels almost doubled during the study period and all patients with signs of FID at baseline responded with an increase in Hb >2g/dL in the IV iron group. TSAT levels reflect iron availability. TSAT levels were below 20% during the treatment period in 27/30 patients (86%) in the non-iron group in comparison with only 3/27 patients (11%) in the IV group. These results indicate that the superior Hb response in the intravenous iron group was due to better availability of iron. Reticulocytes. Hedenus M et al. Leukemia")
43
43-årig menstruerande kvinna, yogalärare
Mångårig blodgivare. Senast augusti 2012. 4/ Hb 86 g/L , Hypokromasi Microcytos Ferritin 5 mmol/L TSAT 0.06 Till läkarbesöket medförde hon en lista över sina symtom!

44
Kognitiva symtom vid järnbrist:
Trötthet- viker inte av vila eller sömn. Depression - allt är grått och tråkigt, orkar inte engagera mig i något, eller avsluta något. Minskad vitalitet - orkar inte göra nått. Nedsatt koncentrationsförmåga, minne och inlärningsförmåga. Nedsatt sexlust.

45
Kroppsliga symtom vid järnbrist:
Blek hy sköra slemhinnor. Skednaglar. Tunna och spricker helt uppe vid kanten. Glatt tunga som svider och sprickor i mungiporna. Försämrad kontroll av kroppstemparatur - är alltid frusen. Andfådd - både när jag talar och när jag rör på mig. Minskad fysisk kapacitet och uthållighet - och jag som är yogalärare nästan 3 timmar varje dag! Myrkrypningar i benen nattetid. Ser sämre - var tvungen att köpa nya glasögon. Takykardi (puls uppe på 150 i 6 timmar). Pica - allt söt! Jag som ALDRIG äter sött och som hatar kakor och bullar - nu har jag bakat äppelkaka och kanelbullar varje dag - vill inte äta "normal mat".
. Pica - allt söt! Jag som ALDRIG äter sött och som hatar kakor och bullar - nu har jag bakat äppelkaka och kanelbullar varje dag - vill inte äta normal mat .")
46
Tumregel för beräkning av järnbehov
Den totala mängden kroppsjärn (erytrocyter, RES och myoglobin) hos en vuxen är 3-4 g För att varaktigt höja Hb med 10 g/L behövs mg järn (motsvarar innehållet i en blodpåse) Om järnförråden är tomma behövs ytterligare mg järn
 hos en vuxen är 3-4 g. För att varaktigt höja Hb med 10 g/L behövs mg järn (motsvarar innehållet i en blodpåse) Om järnförråden är tomma behövs ytterligare 500 mg järn.")
47
Courtesy of Beguin Y. EHA 20013

48
Hb ITT population N 91 anemiska IBD patienter Järnsulfat
(Duroferon 200mgx2) Järnsackaros (Venofer enligt Dosering formel) Lindgren S et al 2009
 Järnsackaros. (Venofer enligt. Dosering formel) Lindgren S et al")
49
Ferritin ITT population (LOCF) Alla patienter
Ferritin-stegringen motsvaras alltså inte av Hb-stegringen inom studiens ram. Lindgren S et al 2009

50
IV järnbehandling vid järnbrist Molekylvikt, kärn- och molekylstorlek
FERRITIN Järnsackaros Venofer (45 kDa) Järnkarboxymaltos/ Låg-Mw järndextran Ferinject Cosmofer Monofer (150 kDa/72–90 kDa) Geisser P et al. Arzneimittelforschung 1992;42:1439–1452; Kudasheva DS et al. J Inorg Biochem 2004;98:1757–1769 50 50
 Järnkarboxymaltos/ Låg-Mw järndextran. Ferinject. Cosmofer. Monofer. (150 kDa/72–90 kDa) Geisser P et al. Arzneimittelforschung 1992;42:1439–1452; Kudasheva DS et al. J Inorg Biochem 2004;98:1757–")
51
No but must wait 30 min after injection
European IV iron product comparison – Product CosmoFer® 1 (low Mw iron dextran) Ferrlecit® 2 (iron gluconate) Venofer® 3 (iron sucrose) Ferinject® 4 (iron carboxymaltose) Feraheme® 5 (Ferumoxytol) Monofer® 6 (iron isomaltoside 1000) Manufacturer Pharmacosmos Sanofi Aventis Vifor AMAG Carbohydrate Dextran (Branched Polysaccharides) Gluconate (Monosaccharides) Sucrose (Disaccharides) Carboxymaltose Carboxymethyl dextran Isomaltoside 1000 (Unbranched Linear Oligosaccharides) Maximum single dose 20mg/kg 125mg 200mg 15mg/kg Single dose limit: 1000 mg 510 mg Maximum single dose administration in a 80 kg man 1600mg 1000mg Maximum single in a 60 kg woman 1200mg 900mg One dose iron repletion (TDI) Yes No Infusion within 1 hour NA Test dose required Yes/No* No but must wait 30 min after injection Iron concentration (mg/ml) 50 12.5 20 30 100 Vial volume (ml) 2 5 2 and 10 17 1, 5 or 10 1) CosmoFer - Summary of Product Characteristics (SPC) by Vitaline Pharma UK: 2) US Ferrlecit Prescribing Information. Bridgewater, NJ: Sanofi Aventis, Inc, 3) Venofer - Summary of Product Characteristics (SPC) by Syner-Med (Pharmaceutical Products) Ltd: 4) Ferinject - Summary of Product Characteristics (SPC) by Syner-Med ( 5) Feraheme Prescribing Information. AMAG Pharmaceuticals, Lexington, MA, USA 6) Monofer - Summary of Product Characteristics (SPC) by Vitaline Pharma UK Abbreviations: TDI: total-dose infusion NA: not applicable * Test dose in the EU but not in the US © 2009 Pharmacosmos A/S 51
 Ferrlecit® 2. (iron gluconate) Venofer® 3. (iron sucrose) Ferinject® 4. (iron carboxymaltose) Feraheme® 5. (Ferumoxytol) Monofer® 6. (iron isomaltoside 1000) Manufacturer. Pharmacosmos. Sanofi Aventis. Vifor. AMAG. Carbohydrate. Dextran. (Branched. Polysaccharides) Gluconate. (Monosaccharides) Sucrose. (Disaccharides) Carboxymaltose. Carboxymethyl dextran. Isomaltoside (Unbranched Linear. Oligosaccharides) Maximum single dose. 20mg/kg. 125mg. 200mg. 15mg/kg. Single dose limit: 1000 mg. 510 mg. Maximum single. dose administration. in a 80 kg man. 1600mg. 1000mg. Maximum single. in a 60 kg woman. 1200mg. 900mg. One dose iron repletion (TDI) Yes. No. Infusion within 1 hour. NA. Test dose required. Yes/No* No but must wait 30 min after injection. Iron concentration (mg/ml) Vial volume (ml) and , 5 or 10. 1) CosmoFer - Summary of Product Characteristics (SPC) by Vitaline Pharma UK: 2) US Ferrlecit Prescribing Information. Bridgewater, NJ: Sanofi Aventis, Inc, ) Venofer - Summary of Product Characteristics (SPC) by Syner-Med (Pharmaceutical Products) Ltd: 4) Ferinject - Summary of Product Characteristics (SPC) by Syner-Med ( documentId= ) Feraheme Prescribing Information. AMAG Pharmaceuticals, Lexington, MA, USA 6) Monofer - Summary of Product Characteristics (SPC) by Vitaline Pharma UK Abbreviations: TDI: total-dose infusion. NA: not applicable. * Test dose in the EU but not in the US. © 2009 Pharmacosmos A/S. 51.")
52
”…måste användas med försiktighet vid akut eller kronisk infektion,
astma, eksem atopiska allergier. Det rekommenderas att administrering avbrytes vid pågående bakteriemi.” Ur årets FASS för intravenösa järnpreparat Cave vid samtidig anthracyklin-behandling ?

53
Pat får 1,5 g järn IV 2 månader senare Helt symtomfri Normalt Hb och ferritin

54
Men endast 50-65% svarar på EPO.
Hedenus M et al. J Clin Oncol 2005;23:6941–6948 Darbepoetin alfa Placebo P <0.001 P <0.001 P <0.001 n = 174 n = 86 n = 88 64 60 56 n = 86 Key points Darbepoetin alfa increased the percentage of patients achieving a Hb response to 60%, from 18% in the placebo group (P <0.001).1 When analysed by malignancy type, the difference between response rates in the darbepoetin alfa and placebo groups was significant in each case: lymphoma: darbepoetin alfa 64% vs placebo 13% (P <0.001) myeloma: darbepoetin alfa 56% vs placebo 23% (P <0.001).1 Background Previously published studies have suggested a possible difference in the Hb response rate between patients with multiple myeloma and lymphoma, although more recent studies have not supported this observation.2,3 In the present study, similar rates of response were seen in both sets of patients. References 1. Hedenus M, et al. Br J Haematol. In press. 2. Dammacco F, et al. Br J Haematol. 2001;113: 3. Österborg A, et al. J Clin Oncol. 2002;20: n = 170 n = 84 23 18 13 Overall Lymphoma Myeloma * Hemoglobin response is defined as an increase of 2 g/dL from baseline in the absence of any RBC transfusion within the preceding 28 days
.1. When analysed by malignancy type, the difference between response rates in the darbepoetin alfa and placebo groups was significant in each case: lymphoma: darbepoetin alfa 64% vs placebo 13% (P <0.001) myeloma: darbepoetin alfa 56% vs placebo 23% (P <0.001).1. Background. Previously published studies have suggested a possible difference in the Hb response rate between patients with multiple myeloma and lymphoma, although more recent studies have not supported this observation.2,3 In the present study, similar rates of response were seen in both sets of patients. References. 1. Hedenus M, et al. Br J Haematol. In press. 2. Dammacco F, et al. Br J Haematol. 2001;113: Österborg A, et al. J Clin Oncol. 2002;20: n = 170. n = Overall. Lymphoma. Myeloma. * Hemoglobin response is defined as an increase of 2 g/dL from baseline in the absence of any RBC transfusion within the preceding 28 days.")
59
GUIDELINES EPO vid CIA Submitted for publication

60
IV iron only (LPD CIA) Change Hb g/dL
Hedenus M et al ASH 2013 p=0.004 p=0.03 p=0.005

62
PREFER Evaluderade effekten av en dos i.v. järn dos vid oförklarlig fatigue hos menstruerande friska kvinnor med järnbrist men med Hb > 115 g/L. 294 kvinnor Randomiserd, placebo- kontrollerad, blindad studie Hedenus M et al (EHA), submitted for publication
, submitted for publication.")
63
IV iron treatment rapidly improved fatigue symptoms
PFS = Piper Fatigue Scale p=0.03 Total PFS improved significantly more often in iron-treated patients Total PFS improved significantly 7 days after iron treatment Day 56 after treatment Hedenus M et al (EHA), submitted for publication
, submitted for publication.")
64
Mitt budskap Cancerrelaterad anemi är vanligt bör och kan behandlas
EPO är ofta ett bättre och billigare alternativ än blodtransfusion Järn är viktigt för en effektiv erythropoes Intravenöst järn Ges vid funktionell järnbrist (Tsat<0,5 ferritin<100) Intolerans PO järn vid absolut ID Grav IDA där snabb effekt önskas Potentierar Epo-behandling och gör den kostnadseffektiv Symtomgivande järnbrist utan anemi bör behandlas ?
 Intolerans PO järn vid absolut ID. Grav IDA där snabb effekt önskas. Potentierar Epo-behandling och gör den kostnadseffektiv. Symtomgivande järnbrist utan anemi bör behandlas")
65
Ge järnet ! Tack för uppmärksamheten ! Innan Du ordinerar blod :
Titta på patienten, inte bara på Hb-värdet !!! Överväg alltid andra alternativ Ett bra alternativ är IV järn 65

Liknande presentationer




















>")
 okt-nov 2010 2010-12-18.>")