Ladda ner presentationen
Presentation laddar. Vänta.

1
Multiple Myeloma Hareth Nahi Haematology center, Karolinska, Huddinge

2
Multiplet Myelom Är en cancerform med ursprung ifrån plasmacellerna.
Den betraktas som en kronisk sjukdom, Viktigt att komma ihåg är att många gamla och nya mediciner förlänger livet betydligt och att prognosen har förbättrat för varje år de senare åren

3
Plasmaceller är högspecialiserade antikroppsproducerande
B-celler. Plasmaceller har en mycket hög utsöndring av antikroppar

4
Diagnostiska kriterier
Förekomst av M-komponent och/eller förekomst av lätta kedjor i dygnsurin i kombination med minst ett subnormalt polyklonalt immunglobulin. >10% plasmaceller i benmärgsutstryk typiska skelettförändringar på röntgen.

5
Behandlingsinduktion
1-Hyperkalcemi (höga kalk nivåer) 2-Anemi (blodbrist) 3-Njurpåverkan 4-Skelett engagemang
 2-Anemi (blodbrist) 3-Njurpåverkan. 4-Skelett engagemang.")
6
Genes Inga säkra omgivningsfaktorer

7
Genes Inga säkra omgivningsfaktorer Ålder - Kön - Ras -

8
Genes Inga säkra omgivningsfaktorer
Ålder - risken ökar med åldern, median ~70 år Kön - Ras -

9
Genes Inga säkra omgivningsfaktorer
Ålder - risken ökar med åldern, median ~70 år Kön - Kvinnor/män 40/60 Ras -

10
Genes Inga säkra omgivningsfaktorer
Ålder - risken ökar med åldern, median ~70 år Kön - Kvinnor/män 40/60 Ras - Ovanlig sjukdom bland asiater, 2-3 ggr vanligare bland afrikaner jmf med europeér

11
Genes Inga säkra omgivningsfaktorer
Ålder - risken ökar med åldern, median ~70 år Kön - Kvinnor/män 40/60 Ras - Ovanlig sjukdom bland asiater, 2-3 ggr vanligare bland afrikaner jmf med europeér Arv /år X 30 år= 0.6% ”Det är inte ditt fel”

12
International Staging System Stage ISS Criteria I
Durie-Salmon system: widely used since 1975 Stage based on M-protein levels, bone lesions, Hb values, serum calcium International Staging System Stage ISS Criteria I β2-microglobulin < 3.5; albumin ≥ 3.5 II Neither stage I nor stage III values III β2-microglobulin > 5.5

13
Prognostiska faktorer
Nedsatt njurfunktion. 2. Beta-2 mikroglobulin, stegrat vid diagnos 3. Vissa kromosomrubbningar

15
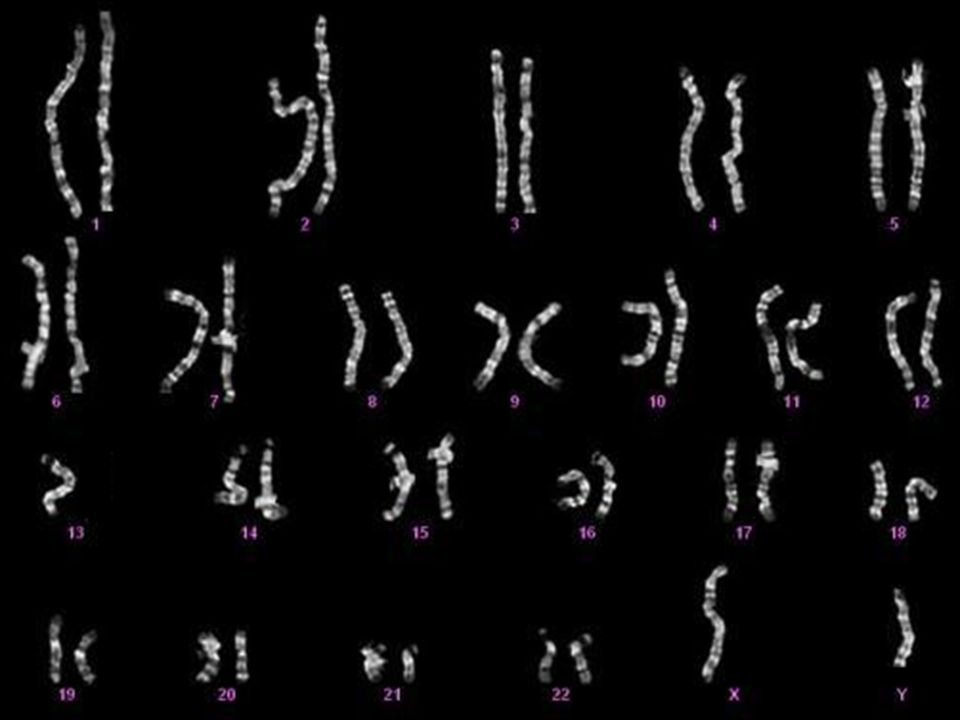
The prognostic significance of 8p21 deletion in multiple myeloma
Tolga Sutlu, Gösta Gahrton and Hareth Nahi Despite the progress in multiple myeloma (MM) therapy (Bjorkstrand and Gahrton 2007), almost all patients treated with autologous stem cell transplantation (ASCT) relapse due to residual disease (Alici, et al 2007). Factors that predict survival in MM including β2-microglobulin (β2M), creatinine and haemoglobin (Hb) levels have been well defined (Durie, et al 2003). Furthermore, the occurrence of various chromosomal abnormalities among the malignant cells (Avet-Loiseau, et al 2007) such as del(13), t(4;14), t(11;14), del(17p), t(14;16), t(14:20), and 1q gains have been shown to have an impact on prognosis. Nevertheless, better assessment and stratification of prognostic factors are needed in order to comprehend the different responses to therapy. Information gained this way will enhance the understanding about treatment prediction in patients with MM. In this study, we analyzed various chromosomal regions by FISH in bone marrow (BM) aspirations from newly diagnosed patients with MM and discovered that loss of the 8p21 region is an independent prognostic factor. Division of Hematology, Department of Medicine Karolinska University Hospital Huddinge 15
 therapy (Bjorkstrand and Gahrton 2007), almost all patients treated with autologous stem cell transplantation (ASCT) relapse due to residual disease (Alici, et al 2007). Factors that predict survival in MM including β2-microglobulin (β2M), creatinine and haemoglobin (Hb) levels have been well defined (Durie, et al 2003). Furthermore, the occurrence of various chromosomal abnormalities among the malignant cells (Avet-Loiseau, et al 2007) such as del(13), t(4;14), t(11;14), del(17p), t(14;16), t(14:20), and 1q gains have been shown to have an impact on prognosis. Nevertheless, better assessment and stratification of prognostic factors are needed in order to comprehend the different responses to therapy. Information gained this way will enhance the understanding about treatment prediction in patients with MM. In this study, we analyzed various chromosomal regions by FISH in bone marrow (BM) aspirations from newly diagnosed patients with MM and discovered that loss of the 8p21 region is an independent prognostic factor. Division of Hematology, Department of Medicine. Karolinska University Hospital Huddinge. 15.")
16
The study FISH analysis: 1q21 8p21 19q13 17p13 15q22 6q21 13q14.3
Number of Patients 58 Age (years) 58 (36-72) Time to ASCT (months) 5,3 (0,7-15,7) Plasma cells (% in BM) 23 (10-80) Hb (g/L) 115 ( ) Creatinine (umol/L) 94 (38-980) β2M (mg/L) 2,7 (0,9-18) Stage ( 1/2/3) 1 / 12 / 45 FISH analysis: 1q21 8p21 19q13 17p13 15q22 6q21 13q14.3 t(4;14) t(11;14) Statistical analysis Survival curves Multivariate analysis of prognostic factors Clustering of chromosomal aberrations This study was approved by the local research ethics committee. Bone marrow aspirations were analysed from 65 patients with MM at diagnosis. The mean age was 56 years (range 36-72). 58 of these patients were then subjected to a standard treatment protocol including debulking with 2-4 cycles of VAD (vincristine, doxorubicin, betametason) followed by high dose treatment and autologous stem cell transplantation (ASCT). Stem cells were harvested by leukapheresis after mobilization using granulocyte-colony stimulating factor and cyclophosphamide. The conditioning regimen was melphalan 200mg/m2. Patient characteristics are given in Table 1. FISH analysis was performed using the following probes: 1q21/8p21, 19q13/17p13, 15q22/6q21 dual colour probe sets from MP Biomedicals, Illkirch, France. 13q14.3 deletion probe (13qter clone 163c9) from Cytocell, Cambridge, United Kingdom. LSI 9p21/CEP-9 dual colour probe, LSI IGH/FGFR3 dual fusion translocation probe for t(4;14) and LSI IGH/CCND1 XT dual fusion translocation probe from Abbot Molecular Inc., Illinois, USA. Statistical analysis was done using SPSS 15 software (SPSS Inc. Chicago, Illinois, USA). The variables were analyzed by using Log-rank tests on Kaplan-Meier plots to identify their impacts on progression-free survival (PFS) and overall survival (OS). Bivariate correlations between the occurrences of chromosomal aberrations were analyzed by a two-tailed test of significance using Kendall’s tau-b coefficient. A hierarchical clustering that fits the correlations observed by this method was obtained by using average linkage between groups and the pattern difference as a measure of the distance between factors. Pattern difference is a dissimilarity measure for binary data that is computed from a four-fold table as bc/(n2), where b and c represent the diagonal cells corresponding to cases present on one item but absent on the other and n is the total number of observations. Prognostic factors for survival were also subjected to multivariate analysis using the Cox proportional hazards regression model with forward stepwise method. PFS and OS were defined as the time from the day of ASCT to progression or death and censored at last contact. 16
 58 (36-72) Time to ASCT (months) 5,3 (0,7-15,7) Plasma cells (% in BM) 23 (10-80) Hb (g/L) 115 ( ) Creatinine (umol/L) 94 (38-980) β2M (mg/L) 2,7 (0,9-18) Stage ( 1/2/3) 1 / 12 / 45. FISH analysis: 1q21. 8p21. 19q13. 17p13. 15q22. 6q21. 13q14.3. t(4;14) t(11;14) Statistical analysis. Survival curves. Multivariate analysis of prognostic factors. Clustering of chromosomal aberrations. This study was approved by the local research ethics committee. Bone marrow aspirations were analysed from 65 patients with MM at diagnosis. The mean age was 56 years (range 36-72). 58 of these patients were then subjected to a standard treatment protocol including debulking with 2-4 cycles of VAD (vincristine, doxorubicin, betametason) followed by high dose treatment and autologous stem cell transplantation (ASCT). Stem cells were harvested by leukapheresis after mobilization using granulocyte-colony stimulating factor and cyclophosphamide. The conditioning regimen was melphalan 200mg/m2. Patient characteristics are given in Table 1. FISH analysis was performed using the following probes: 1q21/8p21, 19q13/17p13, 15q22/6q21 dual colour probe sets from MP Biomedicals, Illkirch, France. 13q14.3 deletion probe (13qter clone 163c9) from Cytocell, Cambridge, United Kingdom. LSI 9p21/CEP-9 dual colour probe, LSI IGH/FGFR3 dual fusion translocation probe for t(4;14) and LSI IGH/CCND1 XT dual fusion translocation probe from Abbot Molecular Inc., Illinois, USA. Statistical analysis was done using SPSS 15 software (SPSS Inc. Chicago, Illinois, USA). The variables were analyzed by using Log-rank tests on Kaplan-Meier plots to identify their impacts on progression-free survival (PFS) and overall survival (OS). Bivariate correlations between the occurrences of chromosomal aberrations were analyzed by a two-tailed test of significance using Kendall’s tau-b coefficient. A hierarchical clustering that fits the correlations observed by this method was obtained by using average linkage between groups and the pattern difference as a measure of the distance between factors. Pattern difference is a dissimilarity measure for binary data that is computed from a four-fold table as bc/(n2), where b and c represent the diagonal cells corresponding to cases present on one item but absent on the other and n is the total number of observations. Prognostic factors for survival were also subjected to multivariate analysis using the Cox proportional hazards regression model with forward stepwise method. PFS and OS were defined as the time from the day of ASCT to progression or death and censored at last contact. 16.")
17
Chromosomal aberrations
Incidence PFS (months) OS (months) deletions 13q14 35 (60%) 50 vs. 15* NR vs. 45* 8p21 14 (24%) 27 vs. 12* 67 vs. 24* 6q21 5 (9%) 22 vs. 14 57 vs. 32 17p13 13 (22%) 21 vs. 26 52 vs. NR amplifications 1q21 22 (38%) 79 vs. 45 15q22 29 (50%) 21 vs. 20 52 vs. 57 19q13 24 (41%) 21 vs. 22 52 vs. 41 9p21 21 (36%) 22 vs. 21 52 vs. 67 locations Trans t(4;14) 9 (15%) 22 vs. 18 57 vs. 34 t(11;14) 8 (14%) 52 vs. 79 ALL 58 22 52 According to univariate analysis del(13)(q14), amp(1)(q21) and del(8)(p21) were significantly associated with PFS while only del(13)(q14) and del(8)(p21) had significant effect on OS. Other factors such as t(4;14) (57 months vs. 34 months, p>0.05) which have been shown to have effect on survival did not present any significance in this series. This is possibly due to the fact that a larger number of patients is needed to investigate the effect of events with such low incidence (10-15%) (Avet-Loiseau, et al 2007), whereas del(8)(p21) seems to have a higher incidence (24%) in this series. 17
 OS (months) deletions. 13q (60%) 50 vs. 15* NR vs. 45* 8p (24%) 27 vs. 12* 67 vs. 24* 6q21. 5 (9%) 22 vs vs p (22%) 21 vs vs. NR. amplifications. 1q (38%) 79 vs q (50%) 21 vs vs q (41%) 21 vs vs p (36%) 22 vs vs. 67. locations. Trans. t(4;14) 9 (15%) 22 vs vs. 34. t(11;14) 8 (14%) 52 vs. 79. ALL According to univariate analysis del(13)(q14), amp(1)(q21) and del(8)(p21) were significantly associated with PFS while only del(13)(q14) and del(8)(p21) had significant effect on OS. Other factors such as t(4;14) (57 months vs. 34 months, p>0.05) which have been shown to have effect on survival did not present any significance in this series. This is possibly due to the fact that a larger number of patients is needed to investigate the effect of events with such low incidence (10-15%) (Avet-Loiseau, et al 2007), whereas del(8)(p21) seems to have a higher incidence (24%) in this series. 17.")
18
Myelom – klinisk bild Benmärgsinsufficiens ger trötthet
Skelettdestruktioner ger värk Hypogammaglobulinemi ger infektionskänslighet Risk för njursvikt

19
ß2M <2.5 / 2.5-5.5 / >5.5 mg/L, % 12 / 55 / 33
Man/Kvinna, % /49 Median ålder, år Ålder ≥75 år, % ß2M <2.5 / / >5.5 mg/L, % / 55 / 33 IgG / IgA / Lätta Kedjor, % / 24 / 8 Skelett engag., % % plasmaceller i benmärgen Krea. (njurvärdet), CrCl ≤30 / >30-60 / >60 ml/min, % / 48 / 46 Njursvikt/lätt nedsatt/normal Nahi et al, Huddinge, 1500 patients since 1990
, CrCl ≤30 / >30-60 / >60 ml/min, % 6 / 48 / 46. Njursvikt/lätt nedsatt/normal. Nahi et al, Huddinge, 1500 patients since")
20
Progress in the treatment of MM over the past 40 years
1995 onward Tandem ASCT Melphalan From 1980s Myeloablation + ASCT 1962 Prednisone + melphalan 1990s Supportive care 1999 First report on thalidomide April 2004 Bortezomib EU licence April Bortezomib approved for first relapse in Europe 2006 MPT Phase III trials 2007 MPV Phase III and bortezomib front-line trials 2007 Len/dex approved for first relapse in Europe 1995 onward Tandem ASCT

21
Oral protease inhibitor
Progress in the treatment of MM over the past 5 years Pomalidomide Bendamustine Panobinostat Anti CD138 ICAM Antibody Carfilzomib Oral protease inhibitor HDAC Inhibitor Maintenance ??????????? ???????

22
Median overall survival (months)
Year of diagnosis Median overall survival (months) 10 60 70 20 30 40 50 1971–1976 1977–1982 1983–1988 1989–1994 1995–2000 2000–2006 Kumar et al. Blood 2007;110: (Abstract 3594)
 – – – – – –2006. Kumar et al. Blood 2007;110: (Abstract 3594)")
23
Behandling av myelom stadium II och III
>= 70 år p.o. Alkeran+Deltison (MP) var 4:e eller var 6:e vecka ± Thalidomid, alt. MPV Velcade/Kortison Revlimid/Kortison <70 år Om samtidig, annan, sjuklighet eller pat kan bedömas ej var aktuell för högdosterapi, se ovan. Annars behandling till remission (CR eller PR) och därefter högdosterapi
 var 4:e eller var 6:e vecka ± Thalidomid, alt. MPV. Velcade/Kortison. Revlimid/Kortison. <70 år. Om samtidig, annan, sjuklighet eller pat kan bedömas ej var aktuell för högdosterapi, se ovan. Annars behandling till remission (CR eller PR) och därefter högdosterapi.")
24
De Vanligaste biverkningarna
Bortezomib Thalidomide Lenalidomide PN (perifer neuropati) ja Oftast går tillbaka efter avslutad behandling Ja Kan vara bestående nej DVT, djupventrombos sällan PE, lungemboli DVT och LE profylax nödvändig – ja* Thrombocytopenia (låga trombocyter) Neutropenia (låga vita) Gastrointestinal (magtarm biverkn.) Teratogenic (fosterskadande) *In combination with Dex and/or chemotherapy and ESAs
 ja. Oftast går tillbaka efter avslutad behandling. Ja. Kan vara bestående. nej. DVT, djupventrombos. sällan. PE, lungemboli. DVT och LE profylax nödvändig. – ja* Thrombocytopenia. (låga trombocyter) Neutropenia (låga vita) Gastrointestinal. (magtarm biverkn.) Teratogenic (fosterskadande) *In combination with Dex and/or chemotherapy and ESAs.")
25
Pågående kliniska prövningar
Karolinska, Huddinge Industri finansierat Prövar initierat På uppdrag av nordiska gruppen

26
Underhållsstudie med Bortezomib (Velcade) + Skelett studien
Patienter som genomgått högdosbehandling och autolog benmärgstransplantation Slut inkluderat >300 patienter inkluderade Nordiska gruppen Pågår Företags sponsrad

27
Lenalidomid (Revlimid)+Kortison jmf med MPT
Patienter som är inte aktuella för högdosbehandling Primär behandling Företags sponsrad

28
Vaccinationer Grunden är att bygga ett immunförsvar
Syftet är att förebygga återfall Ej avsedda för en fullutvecklad, behandlingskrävande sjukdom Icke behandlingskrävande patienter med successiv stegring av M-komp. Prövar initierat

29
Velcade+Kortison ↔ Velcade+Kortison+ >1-3 linjersbehandling
Panobinostat >1-3 linjersbehandling Företags sponsrad

30
Revlimid+Kortison ↔ Revlimd+Kortison+ >1-3 linjers behandling
Carfilzomib >1-3 linjers behandling Företags sponsrad

31
Revlimid+Kortison i 2:a linjen Del 2 Revlimid↔ Revlimd+Kortison
REVII Del 1 Revlimid+Kortison i 2:a linjen Del 2 Revlimid↔ Revlimd+Kortison >1-3 linjers behandling Prövar initierat

32
Antikroppar HuMax-CD38 HuMax-CD38 är en human antikropp
som angriper CD38 molekylen Vilken uttrycks på ytan av plasmacellerna Refraktära patienter mot minst 2 behandlinsalternativ CD38 CD138

33
3 kliniska studier med 3 nya preparat startas hösten 2011/
Våren 2012

34
BI-505, a Human Anti–Intercellular Adhesion Molecule-1 Monoclonal Antibody
Efter minst ett återfall BioInvent International AB Svenskt företag

35
Pomalidomid+Kortison ↔ Kortison >3 linjers behandling
Företags sponsrad

36
Initierat av E. Alici, G. Gahrton, H. Nahi
NK cellsprojekt Initierat av E. Alici, G. Gahrton, H. Nahi Stöds av AVRIS, KI

37
NK cells Celler som kan identifiera och döda tumörceller.
Inhibitory receptor NK Activating receptor Celler som kan identifiera och döda tumörceller.

38
Expansion protocol T NK-T NK M E MNC 2-3 weeks

Liknande presentationer







 5. Problem med nedskräpning (fråga 1a) 6. Problem med skadegörelse (fråga 1b)>")











