Ladda ner presentationen
Presentation laddar. Vänta.

1
Respirationsfysiologi
Lund April 2012

2
Patientfall 65 år gammal tidigare somatiskt frisk man (76 kg; 178cm) inkommer på IVA med tilltagande andningssvårigheter efter ca 1 veckas anamnes på luftvägsinfektion. Status vid inkomsten (kl 10.00): AF 32/min; SatO2 90% med O2 10 l/min (oxymask); BT 90/40; HF 115; T 38,5. Arteriell blodgas – v.g. se BGA1. Rtg pulm visar infiltrat i höger ovanlob.
 inkommer på IVA med tilltagande andningssvårigheter efter ca 1 veckas anamnes på luftvägsinfektion. Status vid inkomsten (kl 10.00): AF 32/min; SatO2 90% med O2 10 l/min (oxymask); BT 90/40; HF 115; T 38,5. Arteriell blodgas – v.g. se BGA1. Rtg pulm visar infiltrat i höger ovanlob.")
3
Respirationsfysiologi

4
BGA 1 BGA 2 BGA 3 BGA 4 pH 7,36 7,38 7,19 7,05 paO2 7,6 8 6,5 6,6 paCO2 4,2 4,5 6,9 9 HCO3- 20 19 22 23 BE -4 -5 -7 -7,2 SaO2 90 92 85 Hb 145 132 112 110 Hct 42 36 34 33 Lact 1,5 2,3 3,2 3,5 O2 10 l/min mask FiO2 60 FiO2 80 FiO2 100 AF 28-30 Resp Mode NIV TU/PEEP TK TU 12 IP PEEP 5 AF 20-26 34-36 18 VT 360 450 VE 12,4 12,6 8,1

6
Vad händer i patientens respiratoriska system?

7
Hypoxemi Alveolär hypoventilation Shunt V/Q …. Difussionsproblem
Vad är mest sannolik mekanism i den aktuella situationen?

8
Shunt

9
Shunt Venous admixture Anatomical shunt (extrapulmonary)
Virtual shunt – assumed value of Svo2 Pathological shunt Physiological shunt Venous admixture in healthy subject Venous admixture calculated from mixing equation

10
Shunt Shunt Venous admixture QS CC - Ca = QT CC - CV

11
Shunt och gasutbyte

12
Konsoliderad lungvävnad och
gasutbyte

13
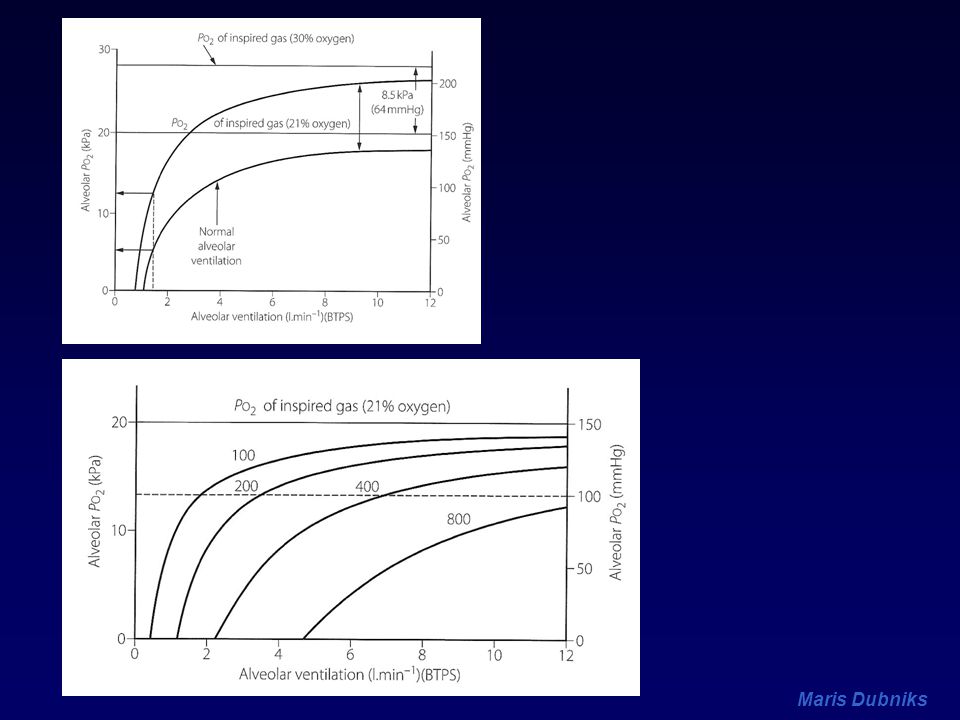
Shunt, FiO2 and PaO2

14
Can we measure the shunt?
PAC – SvO2 The alveolar gas equation – PAO2 ( ) PIO2 - PĒO2 PAO2 = PIO2 - PaCO2 PĒCO2 PIO2 = FIO2 x (PB - PH2O) PH2O = 6.3 kPa (47 mmHg) at t 37O C
 PIO2 - PĒO2. PAO2 = PIO2 - PaCO2. PĒCO2. PIO2 = FIO2 x (PB - PH2O) PH2O = 6.3 kPa (47 mmHg) at t 37O C.")
15
Ventilation Alveolär ventilaton Dead space
VE = VA + VD VA = VE - VD

16
Alveolär ventilation VA = ƒ (VT – VD) VCO2 PaCO2= K VA PaCO2 - ETCO2
VD/VT = PaCO2 VCO2 PaCO2= K VA

17
VCO2 PaCO2= K VA

19
Ventilation, perfusion och V/Q

20
’’Trerumslungan’’

21
Transpulmonellt tryck, luftvägsdiameter och regional fördelning av compliance.

22
Lungperfusion

23
Inverkan av anestesi på ventilation och perfusion

24
V/Q < 1 V/Q > 1 Effects on oxygenatation
Effects on lung mechanics Effects on alveolar dead space and CO2 elimination V/Q > 1 Increases in different pathological situations

25
Compliance Compliance is defined by a volume change per unit of pressure change C = ΔV/ΔP In the normal range of expanding pressures of -2 to -10 cmH2O, normal lung has best compliance At high or low expanding pressures, the lung is stiffer, less compliant

26
Total Compliance

27
Factors influencing Compliance
Increases Deflation (Decremental) Age Emphysema Decreased surface tension Decreases Hi or low lung volume Oedema and fibrosis Atelectasis and consolidation Increased surface tension
 Age. Emphysema. Decreased surface tension. Decreases. Hi or low lung volume. Oedema and fibrosis. Atelectasis and consolidation. Increased surface tension.")
28
Statisk vs. dynamisk compliance

29
FRC Lungornas volym efter normal passiv utandning
Systemets jämviktstillstånd Palv = Patm, inget gasflöde i luftvägar 1/3 del av organismens O2 reserv största del av gasutbyte inträffar vid andningmedelläget beskriver indirekt mekaniska egenskaper och antal av funktionella alveoler

30
FRC – effekt av kroppsläge

31
FRC och CC

32
Luftvägsavstängning Closing Capacity (CC)
CC - lungvolymen där små luftvägar börjar stänga ökar med stigande ålder ingen effekt av anestesi ökar med olika patologiska tillstånd ödem KOL etc.

33
Luftvägsavstängning (Closing Capacity, CC)
V=FRC+VT V=FRC V</=CV 100 VT FRC V CC RV

34
Förhållanden mellan CC och FRC
V/Q 100 VT FRC V CC CC FRC RV Atelektas

35
Atelectasis and Airway closure
Shunt (% CO) Low V/Q (%CO) 20 10 10 R=0.68 P<0.001 5 R=0.57 P0.001 CV-ERV (ml) Atelectasis (cm2) Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anaesthesia. Br J Anaesth 1998; 81: 681–6
 Low V/Q (%CO) R=0.68. P< R=0.57. P CV-ERV (ml) Atelectasis (cm2) Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anaesthesia. Br J Anaesth 1998; 81: 681–6.")
36
Atelectasis and Airway closure
intrapulmonary shunt is correlated to the amount of atelectasis poorly ventilated lung units (‘low VA/Q’) are correlated with airway closure (measured by the difference in closing volume and expiratory reserve volume - CV–ERV). no correlation between CV–ERV and atelectasis. Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anaesthesia. Br J Anaesth 1998; 81: 681–6
 are correlated with airway closure (measured by the difference in closing volume and expiratory reserve volume - CV–ERV). no correlation between CV–ERV and atelectasis. Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anaesthesia. Br J Anaesth 1998; 81: 681–6.")
37
V CC Ålder FRC (sittande) FRC (liggande) FRC (liggande+anestesi)
5 FRC (sittande) 4 FRC (liggande) 3 FRC (liggande+anestesi) 2 1 20 40 60 80 Ålder Inverkan av ålder, kroppsläge och anestesi på FRC och relationen mellan FRC och den lungvolym vid vilken luftvägarna börjar falla samman under utandning (CC).(G.Hedenstierna)
 4. FRC (liggande) 3. FRC (liggande+anestesi) Ålder. Inverkan av ålder, kroppsläge och anestesi på. FRC och relationen mellan FRC och den lungvolym. vid vilken luftvägarna börjar falla samman under. utandning (CC).(G.Hedenstierna)")
38
FRC - inverkan av anestesi
FRC sänkning under anestesi % (under första 3-10 min) stabilt nedsatt efteråt återställas flera timmar efter anestesi med n-m block eller utan - ingen skillnad
 stabilt nedsatt efteråt. återställas flera timmar efter anestesi. med n-m block eller utan - ingen skillnad.")
39
FRC - inverkan av anestesi
FRC sänkning under anestesi minskad volym av hela systemet (luftvägar, alveoler) luftvägsavstängning (CC, Closing Capacity) atelektaser
 luftvägsavstängning (CC, Closing Capacity) atelektaser.")
40
FRC - inverkan av anestesi
Ansvariga mekanismer liggande position (0,5-1,0 l) kraniell förskjutning av diafragma ökad intrathorakal blodvolym minskad muskeltonus
 kraniell förskjutning av diafragma. ökad intrathorakal blodvolym. minskad muskeltonus.")
41
FRC - inverkan av anestesi
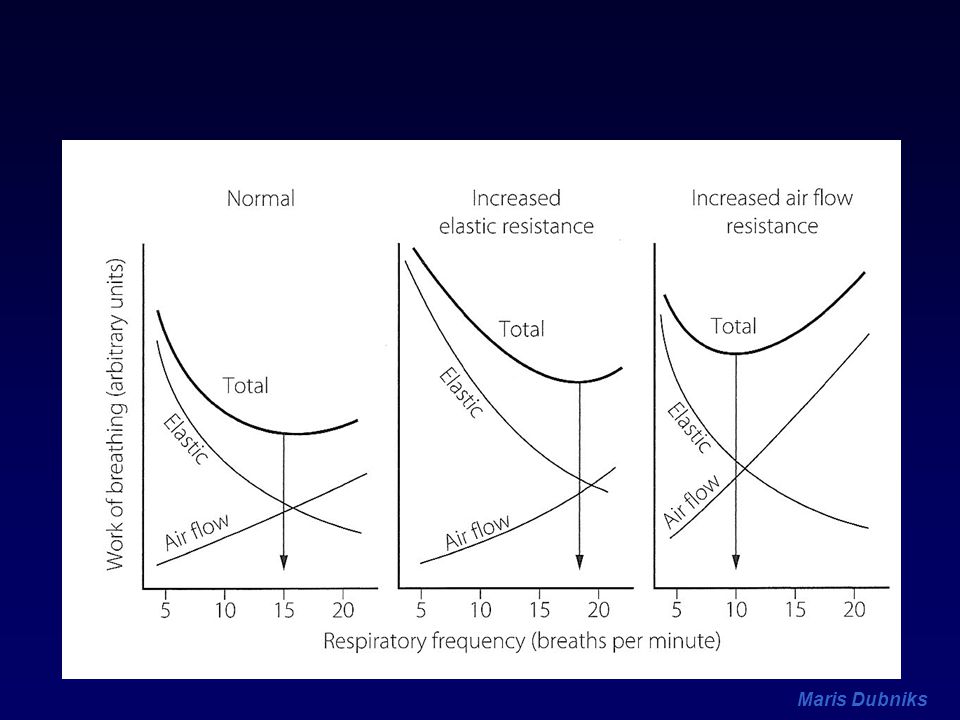
Lungmekanik minskad compliance ökat totalt lungmotstånd (total resistance) Totalt motstånd = luftvägsmot. + vävnadsmot. Trängre luftvägar förändrade elastiska egenskaper ökat muskelarbete (work of breathing) relevant postoperativt
 Totalt motstånd = luftvägsmot. + vävnadsmot. Trängre luftvägar. förändrade elastiska egenskaper. ökat muskelarbete (work of breathing) relevant postoperativt.")
42
FRC och Luftvägsmotstånd

43
Atelektasbildning under anestesi
90% av alla sövda patienter överviktiga har mer KOL patienter har mindre eller inte alls ålder spelar ingen roll Minskad FRC och CC>FRC Kompression Absorbtion (hög FiO2)
")
44
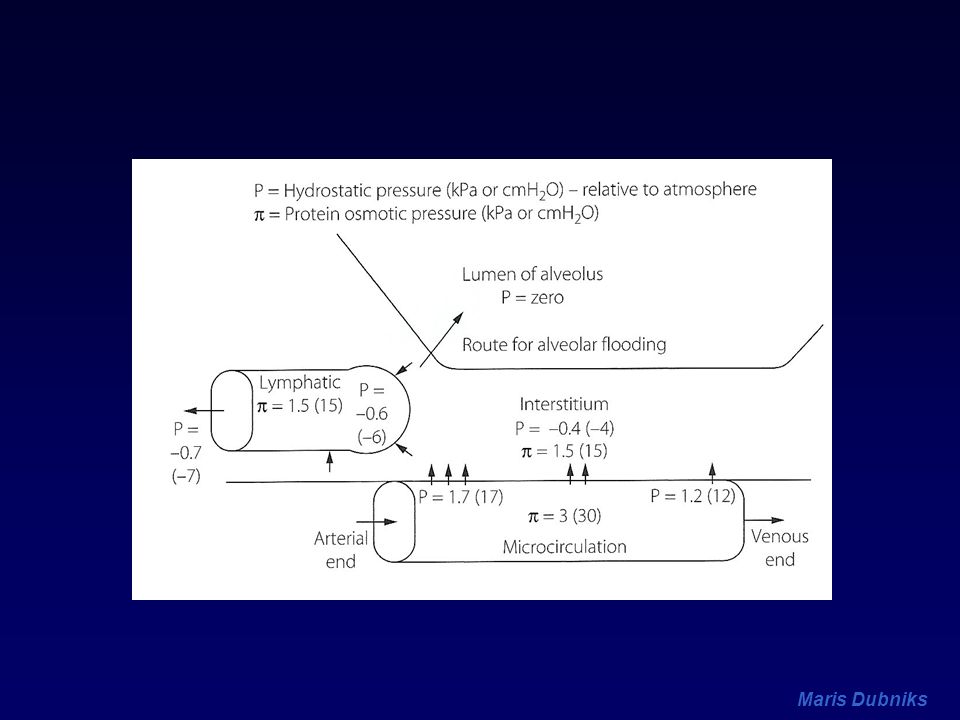
Lungödem Permeabilitetsödem Kardiogent ödem

46
Qf = K (Pc – Pis) - (c - is)
Starling’s equation Qf = K (Pc – Pis) - (c - is) Qf – fluid flux across a membrane P – hydroststic pressure Kf - capillary filtration coefficient - oncotic reflection coefficient - colloid osmotic pressure
 - (c - is) Qf – fluid flux across a membrane. P – hydroststic pressure. Kf - capillary filtration coefficient. - oncotic reflection coefficient. - colloid osmotic pressure.")
47
Hydrostatic Forces Qf = K (Pc – Pis) - (c - is)
 - (c - is)")
48
Vascular permeability
Qf = K (Pc – Pis) - (c - is)
 - (c - is)")
49
Oncotic forces Qf = K (Pc – Pis) - (c - is)
 - (c - is)")
50
Mekanismer Ökad kapillärtryck Ökad permeabilitet
Mitralis stenos, insuffuciens Hjärtsvikt Hypervolemi Ökad permeabilitet Sepsis Inhalation av toxiska substanser Nedsatt lymfatiskt flöde Högt CVP Sänkt interstitiellt tryck Sänkt COP

51
Experimental: Clinical:
Edema begins to form at LAP exceeding mmHg in normal COP; But at 11 mmHg LAP when COP is reduced. Clinical: COP-PAOP gradient has been used to predict mortality Guyton AC Circ Res :649 Rackow EC Chest 1982:43

52
In acute lung injury, any increase in hydrostatic pulmonary capillary pressure increases the amount of plasma traversing the damaged alveolocapillary barrier Increasing left atrial pressure from 3 to 13 mmHg induces an eightfold increase in pulmonary lymphatic flow in dogs with acid-aspiration lung injury as compared to a fourfold increase in animals with normal lungs In patients with ARDS, the transmicrovascular flux of albumin increases proportionally to the microvascular hydrostatic pulmonary pressure calculated from PCWP and pulmonary artery pressure

53
Safety factors Increased lymphatic flow (up tp 10x)
Basal membrane thickening Increased interstitial hydrostatic pressures Decreased interstitial oncotic pressure Activation of epithelial sodium reabsorbtion

54
Lungfunktion Låg complinace Ökad luftvägsresistans Gasutbyte
Interstitiellt ödem har mindre effekt på gasutbyte, ökar områden med låg VA/Q Alveolärt ödem ger hypoxemi pga shunt Hypoxisk vasokonstriktion minskar hypoxemigrad

55
Effect av Pcap on EVLW and PaO2
Noble, Can Anesth Soc J, 1981;27:

56
Lung function in different stages of pulmonary congestion/edema.
AB congestion BC interstitial edema CD alveolar edema Noble, Can Anesth Soc J, 1981;27:

57
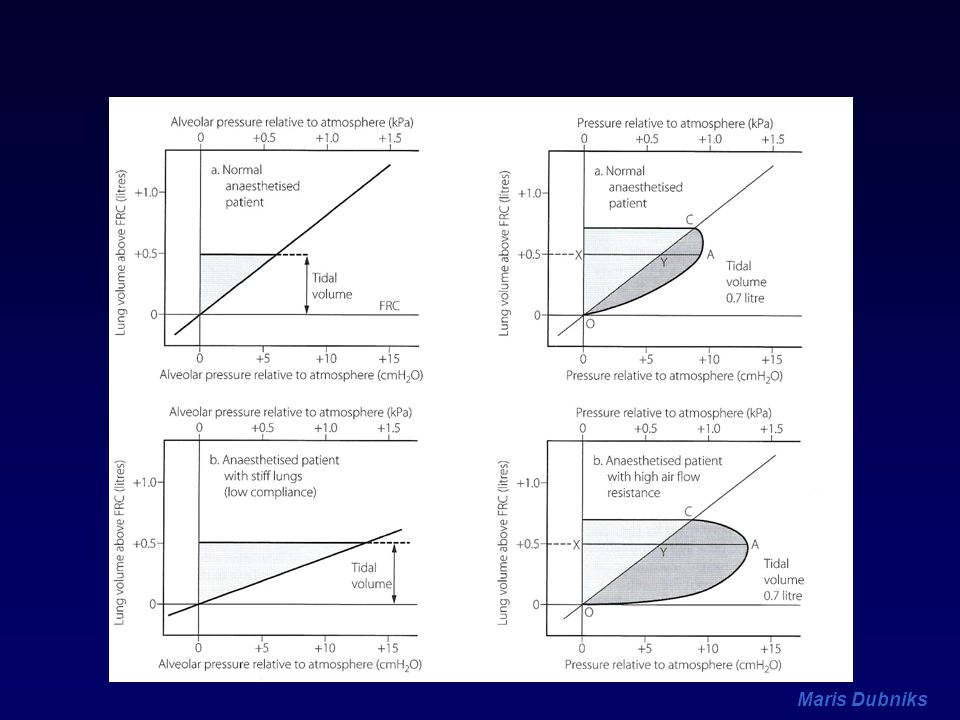
Work of breathing Volume B A1 A Pressure

58
Work of breathing Compliance WOB – Elastic WOB Volume B A1 A Pressure

59
Work of breathing Compliance WOB – Elastic WOB Resistive WOB Volume
Airway resistance Tissue resistance Volume B A1 A Pressure

60
LV FRC P

61
LV FRC P

62
LV FRC P

66
V 1. VT P Relationship between FRC, lung compliance, and work of
breathing: effects of PEEP/CPAP VT A FRCA P

67
V 1. 2. VT VT P Relationship between FRC, lung compliance, and work of
breathing: effects of PEEP/CPAP 2. VT A FRCA VT B FRCB P

68
V 1. 2. VT VT VT P Relationship between FRC,
lung compliance, and work of breathing: effects of PEEP/CPAP 2. VT VT A FRCA C FRCC VT B FRCB P PEEP

69
PEEP effekter Ökar FRC (alveoler och luftvägar)
Förhindrar alveolär kollaps Öppnar kollaberade alveoler Minskar expiratorisk luftvägsavstängning Motverkar mot dynamisk kompression (skillnad) Effekt på V/Q, gasutbyte (hypoxemi) (VD) Effekt på compliance och luftvägsmotstånd Effekt på andningsarbete och VO2resp Protektiv effekt (VILI)
 Effekt på V/Q, gasutbyte (hypoxemi) (VD) Effekt på compliance och luftvägsmotstånd. Effekt på andningsarbete och VO2resp. Protektiv effekt (VILI)")
70
PEEP/CPAP vid lungödem
Fördelning av ekstravaskulärt lungvatten. Bedenberg CE. Ann Thorac Surg Hopewell PC. Am Rev Respir Dis 1979. +10

72
Patientfall Under de närmaste 2 timmarna behandlas patienten med NIV: TU 8/5, FiO2 60%. Vg se BGA2 (kl ). Samtidigt visar patienten tecken till cirkulatorisk instabilitet, ffa i form av lågt BT och stigande laktat. Patienten har fått hittills 2000 ml RA. Behandlande läkare ordinerar ytterligare vätska och under nästa 3 timmar patienten får 3000 ml RA och 500 ml 5% Albumin som inte leder till önskad cirkulatorisk effekt. Noradrenalin infusion påbörjas. Patientens respiratoriska tillstånd försämras ytterligare trots ändringar i NIV inställningar, vg se BGA3. Patienten sövs (Fentanyl, Propofol, Celocurin) och intuberas. I samband med intubationen desatureras patient till 50%. Efter intubationen är pat svårsyresatt, svårventilerad, cirkulatoriskt extremt instabil; se BGA 4.
. Samtidigt visar patienten tecken till cirkulatorisk instabilitet, ffa i form av lågt BT och stigande laktat. Patienten har fått hittills 2000 ml RA. Behandlande läkare ordinerar ytterligare vätska och under nästa 3 timmar patienten får 3000 ml RA och 500 ml 5% Albumin som inte leder till önskad cirkulatorisk effekt. Noradrenalin infusion påbörjas. Patientens respiratoriska tillstånd försämras ytterligare trots ändringar i NIV inställningar, vg se BGA3. Patienten sövs (Fentanyl, Propofol, Celocurin) och intuberas. I samband med intubationen desatureras patient till 50%. Efter intubationen är pat svårsyresatt, svårventilerad, cirkulatoriskt extremt instabil; se BGA 4.")
73
BGA 1 BGA 2 BGA 3 BGA 4 pH 7,36 7,38 7,19 7,05 paO2 7,6 8 6,5 6,6 paCO2 4,2 4,5 6,9 9 HCO3- 20 19 22 23 BE -4 -5 -7 -7,2 SaO2 90 92 85 Hb 145 132 112 110 Hct 42 36 34 33 Lact 1,5 2,3 3,2 3,5 O2 10 mask FiO2 60 FiO2 80 FiO2 100 AF 28-30 Resp Mode NIV TU/PEEP TK TU 12 IP PEEP 5 AF 20-26 34-36 18 VT 360 450 VE 12,4 12,6 8,1

74
Varför allting blir bara sämre?

75
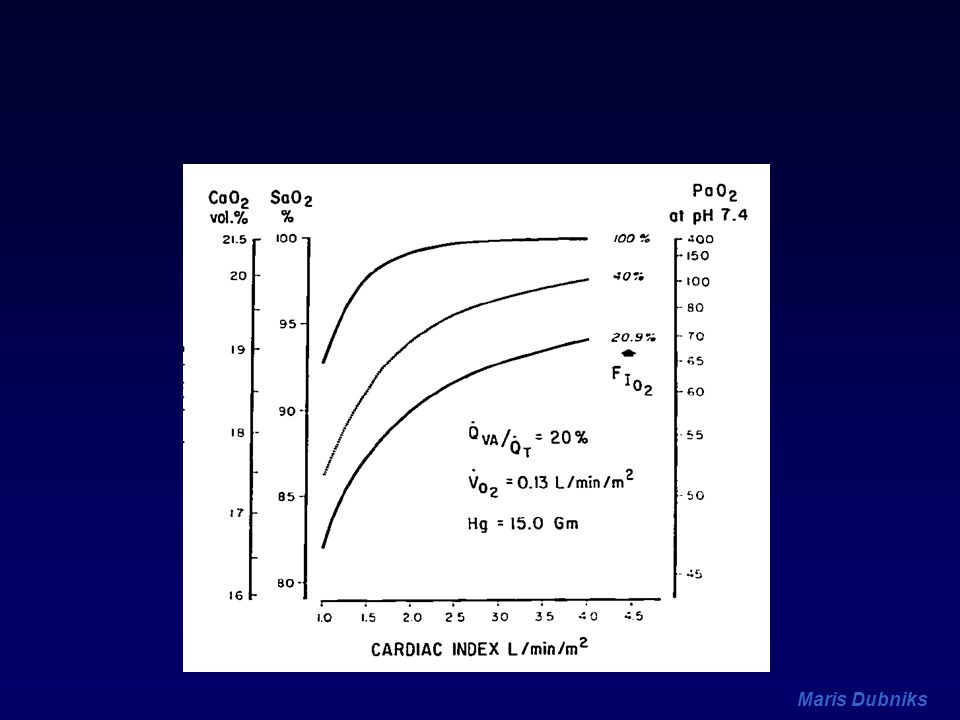
Oxygenering och hjärtminutvolym

78
Två hypoxemi-utlösande mekanismer: låg V/Q och låg PvO2

79
Shunt, cardiac output and oxygenation
Qs/Qt

82
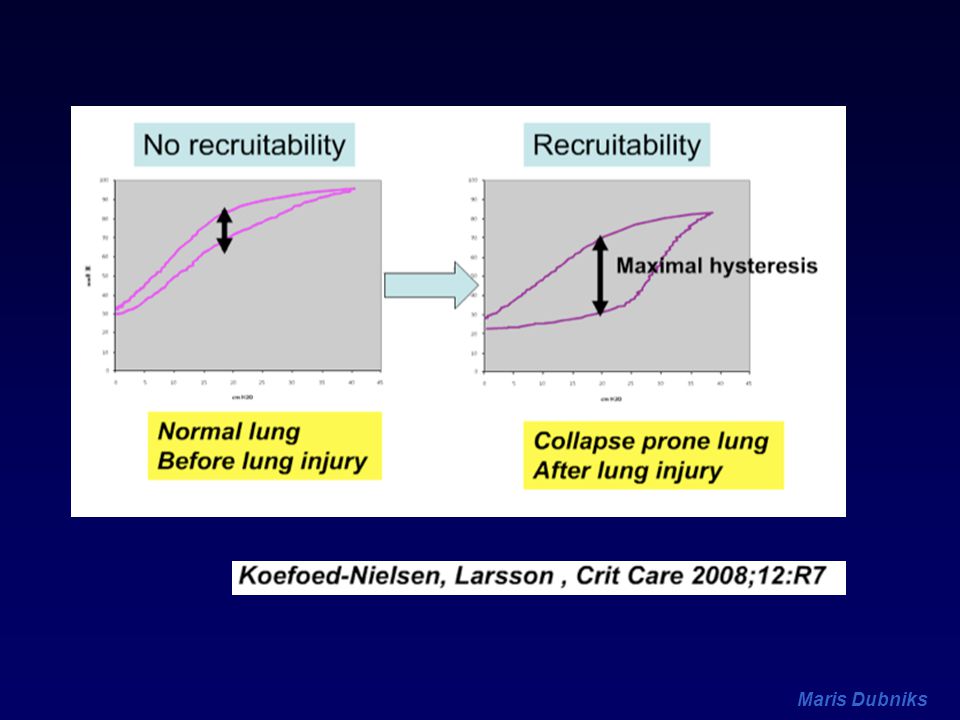
A B C B C A Alveolär kollaps, volutrauma, biotrauma och VILI. V=FRC
V=FRC+1/xVT C B C A V=FRC+VT P2 P1 P

83
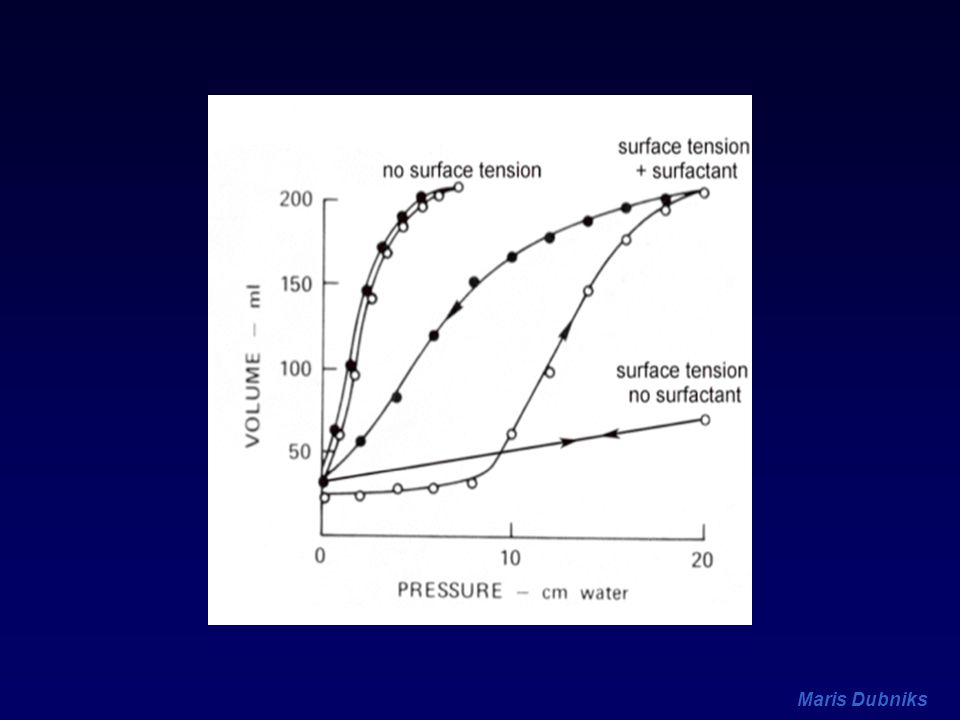
La Place lag P = 2r V P

84
‘’buying time manouver’’ Ashbough 1967
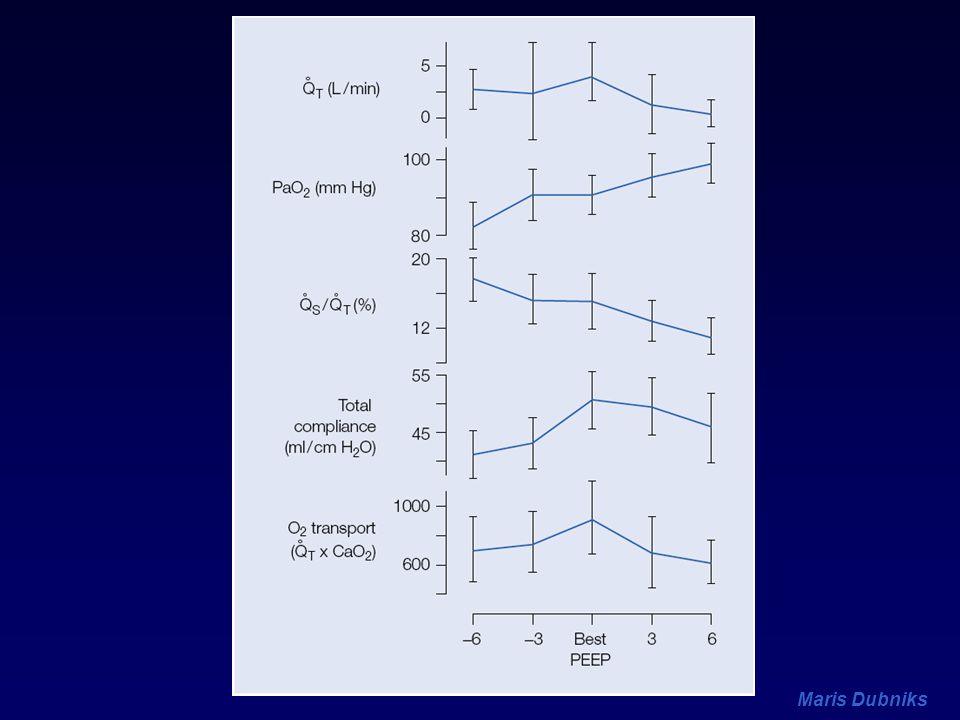
PEEP Suter et al VD/VT; Qs/Qt; Crs; DO2 Optimal PEEP Kirby et al Reduction Qs/Qt 15% Super-PEEP Demers et al Highest SvO2 Best PEEP Caroll et al PaO2>60 with FIO2<60 Minimal PEEP ‘’buying time manouver’’ Ashbough 1967

85
N Eng J Med 1975; 292: The end-expiratory pressure resulting in maximum oxygen transport and the lowest dead space fraction bothe resulted in the greatest total static compliance The end-expiratory pressure varied between 0 and 15 cmH2O and correlated inversely with FRC at ZEEP.

86
Optimum PEEP P Suter NEJM 1075

88
Maisch s et al. An An 2008; 106:175

89
Dynamisk Compliance

90
Dynamisk Compliance

94
Hypoxaemia during induction
The normal store of oxygen is approximately 1500 ml may be increased to 3700 ml with preoxygenation with 100% oxygen. 50% this increase is from the increase in the oxygen concentration in the FRC Farmery AD, Roe PG. Br J Anaesth 1996; 76: 284–91

95
dPpl/dPaw Pinsky MR Curr Op Crit Care 2002

96
Transmural wall tension Chamber radius Systolic pressure
T = Pr Transmural wall tension P.r = 2h Chamber radius Systolic pressure (transmural) Ventricular Volume ITP Pleural pressure Outflow impedance Vascular Compliance Vascular Resistance
 Ventricular Volume. ITP. Pleural pressure. Outflow impedance. Vascular Compliance. Vascular Resistance.")
97
Manipulating DO2 Initial state Transfusion FiO2 or PEEP Crystalloid Inotropes Hb SaO EDVI EF HR DO2I % increase

Liknande presentationer



















 kan användas för att analysera sin miljö.>")


![DANIEL STEINHOLTZ, WWW.ALLIES.SE. ”FRANKLY, WE NEED A REVOLUTION…” [ MAURICE STRONG AT STOCKHOLM +40 ]](/8/2534147/big_thumb.jpg "DANIEL STEINHOLTZ, WWW.ALLIES.SE. ”FRANKLY, WE NEED A REVOLUTION…” [ MAURICE STRONG AT STOCKHOLM +40 ]>")



 2012-2013 Dennis Nordvall Statistiker/Datamanager,>")